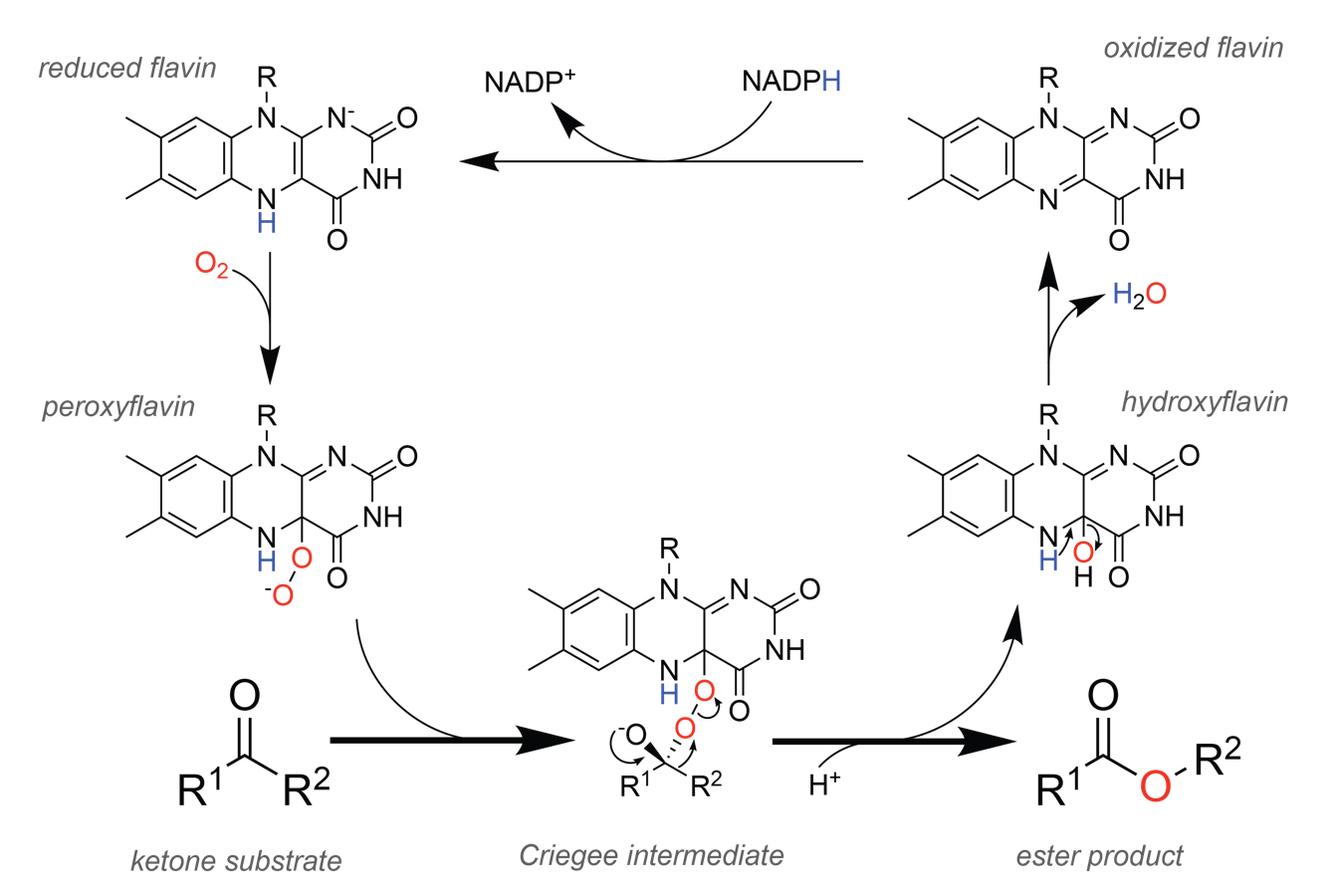
File:BVMO reaction mechanism.png
From HandWiki
Size of this preview: 560 × 376 pixels. Other resolutions: 420 × 282 pixels | 1,342 × 900 pixels.
Original file (1,342 × 900 pixels, file size: 154 KB, MIME type: image/png)
Summary
Submitted to commons.wikimedia.org
Licensing
This file is licensed under the Attribution-Share Alike 3.0 Unported (CC BY-SA 3.0) license. You are free:
- to share – to copy, distribute and transmit the work
- to remix – to adapt the work
Under the following conditions:
- attribution – You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- share alike – If you remix, transform, or build upon the material, you must distribute your contributions under the same or compatible license as the original.
File history
Click on a date/time to view the file as it appeared at that time.
| Date/Time | Thumbnail | Dimensions | User | Comment | |
|---|---|---|---|---|---|
| current | 23:33, 6 October 2025 | | 1,342 × 900 (154 KB) | Maintenance script (talk | contribs) | == Summary == Submitted to commons.wikimedia.org == Licensing == {{CC BY-SA 3.0}} |
You cannot overwrite this file.
File usage
The following page uses this file:


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}