Medicine:Smoking
Smoking is a human behavior which involves the combustion of a substance, usually plant material, and the inhalation of resulting fumes. Today, smoking is mostly practiced by rolling the dried leaves of the tobacco plant into a cigarette. Other forms of tobacco smoking include the use of a smoking tobacco with a pipe or cigar, or using a bong. Cigarette smokers almost always inhale the smoke; most pipe and cigar smokers do not inhale.[1]
Smoking is primarily practiced as a route of administration for psychoactive chemicals because the active substances within the burnt, dried plant leaves (or other chemical) can vaporize into a gaseous state and be delivered into the respiratory tract, where they are rapidly absorbed into the bloodstream through the lungs and can reach the central nervous system. In the case of tobacco smoking, these active substances are a mixture of aerosol particles that include the pharmacologically active alkaloid nicotine, which stimulates the nicotinic acetylcholine receptors in the brain, and other non-psychoactive chemicals that result from combustion. Other notable drugs inhaled via smoking include tetrahydrocannabinol (from cannabis), morphine (from opium), cocaine (from crack), and methamphetamine. Designer drugs, or "research chemicals", can also be smoked.
Tobacco smoking is the most popular form, being practiced by over one billion people globally, of whom the majority are in the developing countries.[2] Less common drugs for smoking include cannabis and opium. Some of the substances are classified as hard narcotics, like heroin, but the use of these is very limited as they are usually not commercially available. Cigarettes are primarily industrially manufactured but also can be hand-rolled from loose tobacco and rolling paper. Other smoking implements include pipes, cigars, bidis, hookahs, and bongs.
Smoking tobacco harms health, and is among the leading causes of many diseases such as lung cancer, heart attack, COPD, erectile dysfunction, and birth defects.[2] Diseases related to tobacco smoking have been shown to kill approximately half of long-term smokers when compared to average mortality rates faced by non-smokers. The World Health Organization (WHO) estimated that smoking killed over seven million smokers worldwide in 2023,[3][4] and 1.6 million non-smokers due to passive smoking.[5] The health risks of smoking have caused many countries to tax tobacco products heavily, publish anti-smoking advertisements and limit or ban tobacco advertising, and help smokers to quit.[2]
Smoking can be dated as early as 5000 BCE, and has been recorded in many different cultures across the world. Early smoking evolved in association with religious ceremonies; as offerings to deities; in cleansing rituals; or to allow shamans and priests to alter their minds for purposes of divination or spiritual enlightenment. After the European exploration and conquest of the Americas, the practice of smoking tobacco quickly spread to the rest of the world. In regions like India and Sub-Saharan Africa, it merged with existing practices of smoking (mostly of cannabis). In Europe, it introduced a new type of social activity and a form of drug intake which previously had been unknown.
Perception surrounding smoking has varied over time and from one place to another: holy and sinful, sophisticated and vulgar, a panacea and deadly health hazard. By the late 20th century, smoking came to be viewed in a decidedly negative light, especially in Western countries.
Health effects

Smoking is one of the leading preventable causes of deaths globally and is the cause of over 7 million deaths annually, 1.6 million of which are non-smokers who die due to passive smoking.[5] In the United States, about 500,000 deaths per year are attributed to smoking-related diseases and a 2004 study estimated that as much as one-third of China's male population will have significantly shortened lifespans due to smoking.[6] Male and female smokers lose an average of 13.2 and 14.5 years of life, respectively.[7] At least half of all lifelong smokers die earlier as a result of smoking.[8][9] The risk of dying from lung cancer before age 85 is 22.1% for a male smoker and 11.9% for a female current smoker, in the absence of competing causes of death. The corresponding estimates for lifelong nonsmokers are a 1.1% probability of dying from lung cancer before age 85 for a man of European descent, and a 0.8% probability for a woman.[10] Smoking just one cigarette a day results in a risk of coronary heart disease that is halfway between that of a heavy smoker and a non-smoker.[11][12] The non-linear dose–response relationship may be explained by smoking's effect on platelet aggregation.[13]
Among the diseases that can be caused by smoking are vascular stenosis, lung cancer,[14] heart attacks[15] and chronic obstructive pulmonary disease (COPD).[16] Smoking during pregnancy may cause ADHD to a fetus.[17]
Smoking is a risk factor strongly associated with periodontitis and tooth loss.[18] The effects of smoking on periodontal tissues depend on the number of cigarettes smoked daily and the duration of the habit. A study showed that smokers had 2.7 times and former smokers 2.3 times greater probabilities to have established periodontal disease than non‐smokers, independent of age, sex and plaque index,[19] however, the effect of tobacco on periodontal tissues seems to be more pronounced in men than in women.[19] Studies have found that smokers had greater odds for more severe dental bone loss compared to non‐smokers;[20] also, people who smoke and drink alcohol heavily have much higher risk of developing oral cancer (mouth and lip) compared with people who do neither.[21] Smoking can also cause milanosis in the mouth.[22]
Smoking has been also associated with oral conditions including dental caries, dental implant failures, premalignant lesions, and cancer.[23] Smoking can affect the immune-inflammatory processes which may increase susceptibility to infections; it can alter the oral mycobiota and facilitate colonization of the oral cavity with fungi and pathogenic molds.[24][25]
Many governments are trying to deter people from smoking with anti-smoking campaigns in mass media stressing the harmful long-term effects of smoking. Passive smoking which affects people in the immediate vicinity of smokers, is a major reason for the enforcement of smoking bans. These are laws enforced to stop individuals from smoking in indoor public places, such as bars, pubs and restaurants, thus reducing nonsmokers' exposure to passive smoke.[26] A common concern among legislators is to discourage smoking among minors, with some countries increasing the age a person must be, to buy cigarettes.[27] In 110 countries graphic health warnings are now displayed on cigarette packaging.[28] Tobacco advertising is also sometimes regulated and/or banned to make smoking less appealing.[29]
Despite the many bans, European countries still hold 18 of the top 20 spots, and according to the ERC, a market research company, the heaviest smokers are from Greece, averaging 3,000 cigarettes per person in 2007.[30] Rates of smoking have leveled off or declined in the developed world but continue to rise in developing countries. Smoking rates in the United States have dropped by half from 1965 to 2006, falling from 42% to 20.8% in adults.[31]
Smoking is a risk factor in Alzheimer's disease.[32] While smoking more than 15 cigarettes per day has been shown to worsen the symptoms of Crohn's disease,[33] smoking has been shown to actually lower the prevalence of ulcerative colitis.[34][35]
Smokers are 30-40% more likely to develop type 2 diabetes than non-smokers, and the risk increases with the number of cigarettes smoked.[36] Script error: No such module "owidslider".
-
![Share of deaths from smoking, 2017[37]](/wiki/images/thumb/d/dd/Share-deaths-smoking.png/360px-Share-deaths-smoking.png) Share of deaths from smoking, 2017[37]
Share of deaths from smoking, 2017[37]
![Share of deaths from smoking, 2017[37]](/wiki/File:Share-deaths-smoking.png)
Physiology

Inhaling the vaporized gas form of substances into the lungs is a quick and very effective way of delivering drugs into the bloodstream (as the gas diffuses directly into the pulmonary vein, then into the heart and from there to the brain) and affects the user within less than a second of the first inhalation. The lungs consist of several million tiny bulbs called alveoli that altogether have an area of over 70 m2 (about the area of a tennis court). This can be used to administer useful medical as well as recreational drugs such as aerosols, consisting of tiny droplets of a medication, or as gas produced by burning plant material with a psychoactive substance or pure forms of the substance itself. Not all drugs can be smoked, for example the sulphate derivative that is most commonly inhaled through the nose, though purer free base forms of substances can, but often require considerable skill in administering the drug properly. The method is also somewhat inefficient since not all of the smoke will be inhaled.[38] The inhaled substances trigger chemical reactions in nerve endings in the brain due to being similar to naturally occurring substances such as endorphins and dopamine, which are associated with sensations of pleasure. The result is what is usually referred to as a "high" that ranges between the mild stimulus caused by nicotine to the intense euphoria caused by heroin, cocaine and methamphetamines.[39]
Inhaling smoke into the lungs, no matter the substance, has adverse effects on one's health.[40] The incomplete combustion produced by burning plant material, like tobacco or cannabis, produces carbon monoxide, which impairs the ability of blood to carry oxygen when inhaled into the lungs. There are several other toxic compounds in tobacco that constitute serious health hazards to long-term smokers from a whole range of causes; vascular abnormalities such as stenosis, lung cancer, heart attacks, strokes, impotence, low birth weight of infants born by smoking mothers. 8% of long-term smokers develop the characteristic set of facial changes known to doctors as smoker's face.[41]
Tobacco smoke is a complex mixture of over 5,000 identified chemicals, of which 98 are known to have specific toxicological properties.[42] The most important chemicals causing cancer are those that produce DNA damage since such damage appears to be the primary underlying cause of cancer.[43] Cunningham et al.[44] combined the microgram weight of the compound in the smoke of one cigarette with the known genotoxic effect per microgram to identify the most carcinogenic compounds in cigarette smoke. The seven most important carcinogens in tobacco smoke are shown in the table, along with DNA alterations they cause.
| Compound | Micrograms per cigarette | Effect on DNA | Ref. |
|---|---|---|---|
| Acrolein | 122.4 | Reacts with deoxyguanine and forms DNA crosslinks, DNA-protein crosslinks and DNA adducts | [45] |
| Formaldehyde | 60.5 | DNA-protein crosslinks causing chromosome deletions and re-arrangements | |
| Acrylonitrile | 29.3 | Oxidative stress causing increased 8-oxo-2'-deoxyguanosine | [46] |
| 1,3-butadiene | 105.0 | Global loss of DNA methylation (an epigenetic effect) as well as DNA adducts | [47] |
| Acetaldehyde | 1448.0 | Reacts with deoxyguanine to form DNA adducts | [48] |
| Ethylene oxide | 7.0 | Hydroxyethyl DNA adducts with adenine and guanine | [49] |
| Isoprene | 952.0 | Single and double strand breaks in DNA | [50] |
Smoking tobacco in any form is harmful to health in many ways, in particular associated with lung cancer. A study of the risk of cancers of the lung, upper aerodigestive tract, and bladder found that pipe smokers had 2.2 times higher risk than non-smokers, cigar smokers had 3.0 times the risk, and cigarette smokers had 5.3 times the risk. Effects for each mode of smoking were stronger in current than former smokers, and in inhalers than in non-inhalers.[51]
Psychology
.jpg)
Most tobacco smokers begin during adolescence or early adulthood. Smoking has elements of risk-taking and rebellion, which often appeal to young people. The presence of high-status models and peers may also encourage smoking. Because teenagers are influenced more by their peers than by adults,[53] attempts by parents, schools, and health professionals at preventing people from trying cigarettes are not always successful.
Smokers often report that cigarettes help relieve feelings of stress. However, the stress levels of adult smokers are slightly higher than those of nonsmokers. Adolescent smokers report increasing levels of stress as they develop regular patterns of smoking, and smoking cessation leads to reduced stress. Far from acting as an aid for mood control, nicotine dependency seems to exacerbate stress. This is confirmed in the daily mood patterns described by smokers, with normal moods during smoking and worsening moods between cigarettes. Thus, the apparent relaxant effect of smoking only reflects the reversal of the tension and irritability that develop during nicotine depletion. Dependent smokers need nicotine to remain feeling normal.[54]
In the mid-20th century psychologists such as Hans Eysenck developed a personality profile for the typical smoker of that period; extraversion was associated with smoking, and smokers tended to be sociable, impulsive, risk taking, and excitement-seeking individuals.[55]
In terms of the Big Five personality traits, research has found smoking to be correlated with lower levels of agreeableness and conscientiousness, as well as higher levels of extraversion and neuroticism.[56]
Prevention
Education and counselling by physicians of children and adolescents has been found to be effective in decreasing the risk of tobacco use.[57] Systematic reviews show that psychosocial interventions can help women stop smoking in late pregnancy, reducing low birthweight and preterm births.[58] A 2016 Cochrane review showed that the combination of medication and behavioural support was more effective than minimal interventions or usual care.[59] Another Cochrane review "suggests that neither reducing smoking to quit nor quitting abruptly results in superior quit rates; people could therefore be given a choice of how to quit, and support provided to people who would specifically like to reduce their smoking before quitting."[60]
-
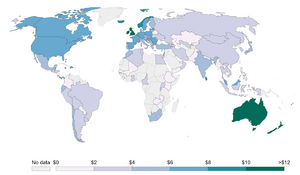 Average price of a pack of 20 cigarettes, measured in international dollars in 2014[61]
Average price of a pack of 20 cigarettes, measured in international dollars in 2014[61] -
![Taxes as a share of cigarette price, 2014[62]](/wiki/images/thumb/d/d4/Taxes-as-share-of-cigarette-price.png/300px-Taxes-as-share-of-cigarette-price.png) Taxes as a share of cigarette price, 2014[62]
Taxes as a share of cigarette price, 2014[62] -
![Types of bans on tobacco advertising, 2014[63]](/wiki/images/thumb/d/d9/Enforcement-of-bans-on-tobacco-advertising.png/300px-Enforcement-of-bans-on-tobacco-advertising.png) Types of bans on tobacco advertising, 2014[63]
Types of bans on tobacco advertising, 2014[63] -
![Support to help quit tobacco use, 2014[64]](/wiki/images/thumb/1/10/Support-to-help-to-quit-tobacco-use.png/300px-Support-to-help-to-quit-tobacco-use.png) Support to help quit tobacco use, 2014[64]
Support to help quit tobacco use, 2014[64]

![Taxes as a share of cigarette price, 2014[62]](/wiki/File:Taxes-as-share-of-cigarette-price.png)
![Types of bans on tobacco advertising, 2014[63]](/wiki/File:Enforcement-of-bans-on-tobacco-advertising.png)
![Support to help quit tobacco use, 2014[64]](/wiki/File:Support-to-help-to-quit-tobacco-use.png)
Prevalence


Smoking is declining. In the year 2000, 32.7% of the global population smoked. By the year 2020, this percentage had decreased to 22.7% of the global population. Smoking is more prevalent in males, with 36.7% of males over the age of 15 smoking, compared to 7.8% of females aged 15 or over. The rate of smoking amongst young people aged 15–24 years has declined from 20.8% in 2000 to 14.2% in 2020. The fastest decline in smoking is in the Americas region, South Asia and Africa are seeing average smoking cessation trends and Europe is seeing slower rates of declines in smoking.[67]
| “ | There is a new Marlboro land, not of lonesome cowboys, but of social-spirited urbanites, united against the perceived strictures of public health.[68] | ” |
History
Early uses

The history of smoking dates back to as early as 5000 BCE for shamanistic rituals.[69] Many ancient civilizations, such as the Babylonian and Chinese, burnt incense as a part of religious rituals, as did the Israelites and the later Catholic and Orthodox Christian churches. Smoking in the Americas probably had its origins in the incense-burning ceremonies of shamans but was later adopted for pleasure, or as a social tool.[70]
Substances such as cannabis, clarified butter (ghee), fish offal, dried snake skins and various pastes molded around incense sticks dates back at least 2000 years. Fumigation (dhupa) and fire offerings (homa) are prescribed in the Ayurveda for medical purposes, and have been practiced for at least 3,000 years while smoking, dhumrapana (literally "drinking smoke"), has been practiced for at least 2,000 years. Before modern times these substances have been consumed through pipes, with stems of various lengths or chillums.[71] Archaeological findings also show the existence of pipes to smoke opium in Cyprus and Crete as soon as the Bronze Age.[72]
Cannabis smoking was common in the Middle East before the arrival of tobacco, and was early on a common social activity that centered around the type of water pipe called a hookah. Smoking, especially after the introduction of tobacco, was an essential component of Muslim society and culture and became integrated with important traditions such as weddings, funerals and was expressed in architecture, clothing, literature and poetry.[73]
Cannabis smoking was introduced to Sub-Saharan Africa through Ethiopia and the east African coast by either Indian or Arab traders in the 13th century or earlier and spread on the same trade routes as those that carried coffee, which originated in the highlands of Ethiopia.[74] It was smoked in calabash water pipes with terracotta smoking bowls, apparently an Ethiopian invention which was later conveyed to eastern, southern and central Africa.
Reports from the first European explorers and conquistadors to reach the Americas tell of rituals where native priests smoked themselves into such high degrees of intoxication that it is unlikely that the rituals were limited to just tobacco.[75]
Popularization

In 1612, six years after the settlement of Jamestown, John Rolfe was credited as the first settler to successfully grow tobacco as a cash crop. The demand quickly grew as tobacco, referred to as "golden weed", revived the Virginia Company from its failed expeditions in search for gold in the Americas.[76] In order to meet demands from the old world, tobacco was grown in succession, quickly depleting the land. This became a motivator to settle west into the unknown continent, and likewise an expansion of tobacco production.[77] Indentured servants became the primary labor force up until Bacon's Rebellion, from which the focus turned to slavery.[78] This trend abated following the American Revolution as slavery became regarded as unprofitable. However, the practice was revived in 1794 with the invention of the cotton gin.[79]
A Frenchman named Jean Nicot (from whose name the word nicotine is derived) introduced tobacco to France in 1560. From France tobacco spread to England. The first report documents an English sailor in Bristol in 1556, seen "emitting smoke from his nostrils".[80] Like tea, coffee and opium, tobacco was just one of many intoxicants that was originally used as a form of medicine.[81]
Soon after its introduction to the Old World, tobacco came under frequent criticism from state and religious leaders. Murad IV, sultan of the Ottoman Empire 1623–40 was among the first to attempt a smoking ban by claiming it was a threat to public morality and health. The Chongzhen Emperor of China issued an edict banning smoking two years before his death and the overthrow of the Ming dynasty. Later, the Manchu rulers of the Qing dynasty, would proclaim smoking "a more heinous crime than that even of neglecting archery". In Edo period Japan, some of the earliest tobacco plantations were scorned by the shōgun as being a threat to the military economy by letting valuable farmland go to waste for the use of a recreational drug instead of being used to plant food crops.[82]

Religious leaders have often been prominent among those who considered smoking immoral or outright blasphemous. In 1634, the Patriarch of Moscow and all Rus' forbade the sale of tobacco and sentenced men and women who flouted the ban to have their nostrils slit and their backs whipped until skin came off their backs. The Western church leader Pope Urban VII likewise condemned smoking in a papal bull of 1590. Despite many concerted efforts, restrictions and bans were almost universally ignored. When James VI and I, a staunch anti-smoker and the author of A Counterblaste to Tobacco, tried to curb the new trend by enforcing an enormous 4000% tax increase on tobacco in 1604; it proved a failure, as London had some 7,000 tobacco sellers by the early 17th century. Later, rulers would realise the futility of smoking bans and instead turned tobacco trade and cultivation into lucrative government monopolies.[83]
By the mid-17th century every major civilization had been introduced to tobacco smoking and in many cases had already assimilated it into its culture, despite the attempts of many rulers to stamp the practice out with harsh penalties or fines. Tobacco, both product, and plant followed the major trade routes to major ports and markets, and then on into the hinterlands. The English language term smoking was coined in the late 18th century; before then the practice was referred to as drinking smoke.[80]
Tobacco and cannabis were used in Sub-Saharan Africa, much like elsewhere in the world, to confirm social relations, but also created entirely new ones. In what is today Congo, a society called Bena Diemba ("People of Cannabis") was organized in the late 19th century in Lubuko ("The Land of Friendship"). The Bena Diemba were collectivist pacifists that rejected alcohol and herbal medicines in favor of cannabis.[84]
The growth remained stable until the American Civil War in the 1860s, from which the primary labor force transition from slavery to sharecropping. This compounded with a change in demand, lead to the industrialization of tobacco production with the cigarette. James Albert Bonsack, a craftsman, in 1881 produced a machine to speed the production of cigarettes.[85]
Opium

In the 19th century, the practice of smoking opium became widespread in China. Previously, opium had only been ingested via consumption, and then only for its medicinal properties (opium was an anaesthetic). The narcotic was also outlawed in China sometime in the early 18th century due the societal issues it caused. Due to a massive trade imbalance, however, foreign merchants started to smuggle opium into China via Canton, to the chagrin of the Chinese authorities. Attempts by Chinese official Lin Zexu to eliminate the trade led to the outbreak of the First Opium War. The Chinese defeat in the First and Second Opium Wars resulted in the legalization of the importation of opium into China.[86][87]
Opium smoking later spread with Chinese immigrants and spawned many infamous opium dens in Chinatowns around South and Southeast Asia, Europe and the Americas. In the latter half of the 19th century, opium smoking became popular in the artistic community in Europe, especially Paris; artists' neighborhoods such as Montparnasse and Montmartre became virtual "opium capitals". While opium dens that catered primarily to emigrant Chinese continued to exist in Chinatowns around the world, the trend among the European artists largely abated after the outbreak of World War I.[86] The consumption of Opium abated in China during the Cultural Revolution in the 1960s and 1970s.[86]
Anti-tobacco movement
Many people have been critical about tobacco use since it gained popularity. In 1798, Dr. Benjamin Rush (early American physician, signer of the Declaration of Independence, Surgeon General under George Washington, and anti-tobacco activist) was "against the habitual use of tobacco" because he believed it (a) "led to a desire for strong drink," (b) "was injurious both to health and morals," (c) "is generally offensive to" nonsmokers, (d) "produces a want of respect for" nonsmokers, and (e) "always disposes to unkind and unjust behavior towards them."[88][89]
With the modernization of cigarette production compounded with the increased life expectancies during the 1920s, adverse health effects began to become more prevalent.[2] In Germany, anti-smoking groups, often associated with anti-liquor groups,[90] first published advocacy against the consumption of tobacco in the journal Der Tabakgegner (The Tobacco Opponent) in 1912 and 1932. In 1929, Fritz Lickint of Dresden, Germany, published a paper containing formal statistical evidence of a lung cancer–tobacco link. During the Great Depression, Adolf Hitler condemned his earlier smoking habit as a waste of money.[91] This anti-smoking movement was further strengthened with Nazi reproductive policy as women who smoked were viewed as unsuitable to be wives and mothers in a German family.[92]
By the end of the Second World War, American cigarette manufacturers quickly reentered the German black market. Illegal smuggling of tobacco became prevalent,[93] and leaders of the Nazi anti-smoking campaign were assassinated.[94] As part of the Marshall Plan, the United States shipped free tobacco to Germany; with 24,000 tons in 1948 and 69,000 tons in 1949.[93] Per capita yearly cigarette consumption in post-war Germany steadily rose from 460 in 1950 to 1,523 in 1963.[95] By the end of the 20th century, anti-smoking campaigns in Germany were unable to exceed the effectiveness of the Nazi-era climax in the years 1939–41 and German tobacco health research was described by Robert N. Proctor as "muted".[95]

In the UK and the US, an increase in lung cancer rates, formerly "among the rarest forms of disease", was noted by the 1930s, but its cause remained unknown and even the credibility of this increase was sometimes disputed as late as 1950. For example, in Connecticut, reported age-adjusted incidence rates of lung cancer among males increased 220% between 1935–39 and 1950–54. In the UK, the share of lung cancer among all cancer deaths in men increased from 1.5% in 1920 to 19.7% in 1947. Nevertheless, these increases were questioned as potentially caused by increased reporting and improved methods of diagnosis. Although several carcinogens were already known at the time (for example, benzo[a]pyrene was isolated from coal tar and demonstrated to be a potent carcinogen in 1933), none were known to be contained in adequate quantities in tobacco smoke.[96] Richard Doll in 1950 published research in the British Medical Journal showing a close link between smoking and lung cancer.[97] Four years later, in 1954 the British Doctors Study, a study of some 40 thousand doctors over 20 years, confirmed the link, based on which the government issued advice that smoking and lung cancer rates were related.[98][99] In 1964 the United States Surgeon General's Report on Smoking and Health demonstrated the relationship between smoking and cancer.[100] Further reports confirmed this link in the 1980s and concluded in 1986 that passive smoking was also harmful.[101]
As scientific evidence mounted in the 1980s, tobacco companies claimed contributory negligence as the adverse health effects were previously unknown or lacked substantial credibility. Health authorities sided with these claims up until 1998, from which they reversed their position. The Tobacco Master Settlement Agreement, originally between the four largest US tobacco companies and the Attorneys General of 46 states, restricted certain types of tobacco advertisement and required payments for health compensation; which later amounted to the largest civil settlement in United States history.[102]
From 1965 to 2006, rates of smoking in the United States have declined from 42% to 20.8%.[103] A significant majority of those who quit were professional, affluent men. Despite this decrease in the prevalence of consumption, the average number of cigarettes consumed per person per day increased from 22 in 1954 to 30 in 1978. This paradoxical event suggests that those who quit smoked less, while those who continued to smoke moved to smoke more light cigarettes.[104] This trend has been paralleled by many industrialized nations as rates have either leveled-off or declined. In the developing countries, however, tobacco consumption continues to rise at 3.4% in 2002.[105] In Africa, smoking is in most areas considered to be modern, and many of the strong adverse opinions that prevail in the West receive much less attention.[106] Today Russia leads as the top consumer of tobacco followed by Indonesia, Laos, Ukraine, Belarus, Greece, Jordan, and China.[107]
At the global scale, initial ideas of an international convention towards the prevention of tobacco had been initiated in the World Health Assembly (WHA) in 1996.[108] In 1998, along with the successful election of Dr. Gro Harlem Brundtland as the Director-General, the World Health Organization set tobacco control as its leading health concern and has begun a program known as the Tobacco Free Initiative (TFI) in order to reduce rates of consumption in the developing world. However, it was not until 2003 that the Framework Convention on Tobacco Control (FCTC) was accepted in WHA and entered into force in 2005. FCTC marked a milestone as the first international treaty concerning a global health issue that aims to combat tobacco in multiple aspects including tobacco taxes, advertisement, trading, environmental affects, health influences, etc.[109] The birth of this evidence-based and systematic approach has resulted in the reinforcement of tobacco taxes and the implementation of smoke-free laws in 128 countries that led to the decrease of smoking prevalence in developing nations.[110] In Nepal, "Smokers are not selfish", a health campaign lasting two weeks is started on the occasion of Valentine's Day and Vasant panchami to motivate individuals to quit smoking as a sacrifice for their loved ones and making it a meaningful decision of life. This campaign is attracting public attention.[111]
Other substances
In the early 1980s, organized international trafficking of cocaine grew. However, overproduction and tighter legal enforcement for the illegal product caused drug dealers to convert the powder to "crack" – a solid, smokable form of cocaine that could be sold in smaller quantities to more people.[112] This trend abated in the 1990s as increased police action coupled with a robust economy caused many potential consumers to give up or fail to take up the habit.[113]
Society and culture
Cigarette smoking, which did not begin to become widespread until the late 19th century, has more associations of modernity and the faster pace of the industrialized world. Cigars have been, and still are, associated with masculinity, power and is an iconic image associated with the stereotypical capitalist. In fact, some evidence suggests that men with higher than average testosterone levels are more likely to smoke.[114] Smoking in public has for a long time been something reserved for men and when done by women has been associated with promiscuity. In Japan during the Edo period, prostitutes and their clients would often approach one another under the guise of offering a smoke; the same was true for 19th-century Europe.[82]
Art

The earliest depictions of smoking can be found on Classical Mayan pottery from around the 9th century. The art was primarily religious in nature and depicted deities or rulers smoking early forms of cigarettes.[115] Soon after smoking was introduced outside of the Americas it began appearing in painting in Europe and Asia. The painters of the Dutch Golden Age were among the first to paint portraits of people smoking and still lifes of pipes and tobacco. For southern European painters of the 17th century, a pipe was much too modern to include in the preferred motifs inspired by mythology from Greek and Roman antiquity. At first smoking was considered lowly and was associated with peasants.[116]
In the 18th century smoking became far more sparse in painting as the elegant practice of taking snuff became popular. Smoking a pipe was again relegated to portraits of lowly commoners and country folk and the refined sniffing of shredded tobacco followed by sneezing was rare in art. When smoking appeared it was often in the exotic portraits influenced by Orientalism. Many proponents of postcolonialism controversially believe this portrayal was a means of projecting an image of European superiority over its colonies and a perception of the male dominance of a feminized Orient. Proponents believe the theme of the exotic and alien "Other" escalated in the 19th century, fueled by the rise in the popularity of ethnology during the Enlightenment.[117]

In the 19th century smoking was common as a symbol of simple pleasures; the pipe smoking "noble savage", solemn contemplation by Classical Roman ruins, scenes of an artist becoming one with nature while slowly toking a pipe. The newly empowered middle class also found a new dimension of smoking as a harmless pleasure enjoyed in smoking saloons and libraries. Smoking a cigarette or a cigar would also become associated with the Bohemian, someone who shunned the conservative middle class values and displayed his contempt for conservatism. But this was a pleasure that was to be confined to a male world; women smokers were associated with prostitution and smoking was not considered an activity fit for proper ladies.[118] It was not until the start of the 20th century that smoking women would appear in paintings and photos, giving a chic and charming impression. Impressionists like Vincent van Gogh, who was a pipe smoker himself, would also begin to associate smoking with gloom and fin-du-siècle fatalism. While the symbolism of the cigarette, pipe and cigar respectively were consolidated in the late 19th century, it was not until the 20th century that artists began to use it fully; a pipe would stand for thoughtfulness and calm; the cigarette symbolized modernity, strength and youth, but also nervous anxiety; the cigar was a sign of authority, wealth and power. The decades following World War II, during the apex of smoking when the practice had still not come under fire by the growing anti-smoking movement, a cigarette casually tucked between the lips represented the young rebel, epitomized in actors like Marlon Brando and James Dean or mainstays of advertising like the Marlboro Man. It was not until the 1970s when the negative aspects of smoking began to appear, yielding the image of the unhealthy lower-class individual, reeking of cigarette smoke and lack of motivation and drive, which was especially prominent in art inspired or commissioned by anti-smoking campaigns.[119]
Film and TV

Ever since the era of silent films, smoking has had a major part in film symbolism. In the hard-boiled film noir crime thrillers, cigarette smoke often frames characters and is frequently used to add an aura of mystique or nihilism.[120]
Since World War II, smoking has gradually become less frequent on screen as the obvious health hazards of smoking have become more widely known. With the anti-smoking movement gaining greater respect and influence, conscious attempts not to show smoking on screen are now undertaken in order to avoid encouraging smoking or giving it positive associations, particularly for family films.[121] Smoking on screen is more common today among characters who are portrayed as anti-social or even criminal.[122]
According to a 2019 study, the introduction of television in the United States led to a substantial increase in smoking, in particular among 16–21-year-olds.[123] The study suggested "that television increased the share of smokers in the population by 5–15 percentage points, generating roughly 11 million additional smokers between 1946 and 1970."[123]
In the United States, a 2019 analysis by the Centers for Disease Control and Prevention of top-grossing films released during 2010–2018 found that, although the number of films with any tobacco imagery remained stable, the total number of tobacco incidents in those films increased by 57%, including a 120% increase in PG-13-rated movies.[124]
The same year, following criticism of smoking depictions in some of its programmes, Netflix announced that future original series rated TV-14 or below and films rated PG-13 or below would not include smoking or e-cigarette use, except where needed for reasons of historical or factual accuracy, and that depictions in higher-rated productions would be limited to cases where smoking was considered essential to the creative vision or characterisation.[125]
A 2022 report from the U.S. public health organisation Truth Initiative on streaming and broadcast television found that 60% of the 15 favourite 2020 season releases for young adults included smoking, and estimated that these programmes exposed about 27 million youths to tobacco imagery.[126]
Literature
Just as in other types of fiction, smoking has had an important place in literature and smokers are often portrayed as characters with great individuality, or outright eccentrics, something typically personified in one of the most iconic smoking literary figures of all, Sherlock Holmes. Other than being a frequent part of short stories and novels, smoking has spawned endless eulogies, praising its qualities and affirming the author's identity as a devoted smoker. Especially during the late 19th century and early 20th century, a panoply of books with titles like Tobacco: Its History and associations (1876), Cigarettes in Fact and Fancy (1906) and Pipe and Pouch: The Smokers Own Book of Poetry (1905) were written in the UK and the US. The titles were written by men for other men and contained general tidbits and poetic musings about the love for tobacco and all things related to it, and frequently praised the refined bachelor's life. The Fragrant Weed: Some of the Good Things Which Have been Said or Sung about Tobacco, published in 1907, contained, among many others, the following lines from the poem A Bachelor's Views by Tom Hall that were typical of the attitude of many of the books:

| “ | So let us drink To her, – but think Of him who has to keep her; And sans a wife Let's spend our life In bachelordom, – it's cheaper. |
” |
| — Eugene Umberger[127] | ||
These works were all published in an era before the cigarette had become the dominant form of tobacco consumption and pipes, cigars, and chewing tobacco were still commonplace. Many of the books were published in novel packaging that would attract the learned smoking gentleman. Pipe and Pouch came in a leather bag resembling a tobacco pouch and Cigarettes in Fact and Fancy (1901) came bound in leather, packaged in an imitation cardboard cigar box. By the late 1920s, the publication of this type of literature largely abated and was only sporadically revived in the later 20th century.[128]
Music
There have been few examples of tobacco in music in early modern times, though there are occasional signs of influence in pieces such as Johann Sebastian Bach's Enlightening Thoughts of a Tobacco-Smoker.[129] However, from the early 20th century and onwards smoking has been closely associated with popular music. Jazz was from early on closely intertwined with the smoking that was practiced in the venues where it was played, such as bars, dance halls, jazz clubs and even brothels. The rise of jazz coincided with the expansion of the modern tobacco industry, and in the United States also contributed to the spread of cannabis. The latter went under names like "tea", "muggles" and "reefer" in the jazz community and was so influential in the 1920s and 30s that it found its way into songs composed at the time such as Louis Armstrong's Muggles, Larry Adler's Smoking Reefers, and Don Redman's Chant of The Weed. The popularity of marijuana among jazz musicians remained high until the 1940s and 50s, when it was partially replaced by the use of heroin.[130]
Another form of modern popular music that has been closely associated with cannabis smoking is reggae, a style of music that originated in Jamaica in the late 1950s and early 60s. Cannabis, or ganja, is believed to have been introduced to Jamaica in the mid-19th century by Indian immigrant labor and was primarily associated with Indian workers until it was appropriated by the Rastafari movement in the middle of the 20th century.[131] The Rastafari considered cannabis smoking to be a way to come closer to God, or Jah, an association that was greatly popularized by reggae icons such as Bob Marley and Peter Tosh in the 1960s and 70s.[132]
Economics
Estimates claim that smokers cost the U.S. economy $97.6 billion a year in lost productivity and that an additional $96.7 billion is spent on public and private health care combined.[133] This is over 1% of the gross domestic product. A male smoker in the United States that smokes more than one pack a day can expect an average increase of $19,000 just in medical expenses over the course of his lifetime. A U.S. female smoker that also smokes more than a pack a day can expect an average of $25,800 additional healthcare costs over her lifetime.[134]
Smoking in the armed forces
The importance of tobacco to soldiers was early on recognized as something that could not be ignored by commanders. By the 17th century allowances of tobacco were a standard part of the naval rations of many nations and by World War I cigarette manufacturers and governments collaborated in securing tobacco and cigarette allowances to soldiers in the field. It was asserted that regular use of tobacco while under duress would not only calm the soldiers but allow them to withstand greater hardship.[135] Until the mid-20th century, the majority of the adult population in many Western nations were smokers and the claims of anti-smoking activists were met with much skepticism, if not outright contempt.[136] Smoking in the armed forces is now discouraged.[137][138] Within the UK Armed Forces, 27% of personnel smoked in 2011, with this declining to 18% by 2020.[139] In the US military, smokers are at higher risk of sustaining injuries in training and of being discharged prematurely.[140]
See also
- Cigarette smoking for weight loss
- Electronic cigarette
- Outline of smoking
- Plain tobacco packaging
- Reverse smoking
- Schizophrenia and tobacco smoking
- Smoke social
- Varenicline
- Smoker's paradox
- Smoking in association football
References
- ↑ Turner, J. A. McM.; Sillett, R. W.; McNicol, M. W. (1 January 1981). "The inhaling habits of pipe smokers". British Journal of Diseases of the Chest 75 (1): 71–76. doi:10.1016/S0007-0971(81)80009-5. ISSN 0007-0971. PMID 7259968.
- ↑ 2.0 2.1 2.2 2.3 "Tobacco Fact sheet N°339". May 2014. https://www.who.int/mediacentre/factsheets/fs339/en/.
- ↑ Ritchie, Hannah; Roser, Max (November 2023), Smoking, https://ourworldindata.org/smoking#the-global-distribution-of-smoking-deaths, retrieved 14 October 2025
- ↑ Lay, Kat (24 June 2025). "Tobacco exposure killed more than 7m people in 2023, study finds". The Guardian. https://www.theguardian.com/society/2025/jun/24/tobacco-exposure-killed-more-than-7m-people-worldwide-2023-study.
- ↑ 5.0 5.1 "Tobacco". World Health Organization. https://www.who.int/en/news-room/fact-sheets/detail/tobacco.
- ↑ Iversen, Leslie (2004). "Why Do We Smoke? The Physiology of Smoking". Smoke: A Global History of Smoking. London: Reaktion Books. pp. 318–321.
- ↑ Centers for Disease Control and Prevention (CDC) (2002). "Annual smoking-attributable mortality, years of potential life lost, and economic costs – United States, 1995–1999". MMWR Morb. Mortal. Wkly. Rep. 51 (14): 300–03. PMID 12002168.
- ↑ "Mortality in relation to smoking: 50 years' observations on male British doctors". BMJ 328 (7455): 1519. 2004. doi:10.1136/bmj.38142.554479.AE. PMID 15213107.
- ↑ "Excess mortality among cigarette smokers: changes in a 20-year interval". Am J Public Health 85 (9): 1223–30. 1995. doi:10.2105/ajph.85.9.1223. PMID 7661229.
- ↑ "Lung cancer occurrence in never-smokers: An analysis of 13 cohorts and 22 cancer registry studies". PLOS Med 5 (9). 2008. doi:10.1371/journal.pmed.0050185. PMID 18788891.
- ↑ Kenneth Johnson (Jan 24, 2018). "Just one cigarette a day seriously elevates cardiovascular risk". British Medical Journal 360: k167. doi:10.1136/bmj.k167. PMID 29367307.
- ↑ "Just one cigarette a day can cause serious heart problems". New Scientist. Feb 3, 2020. https://www.newscientist.com/article/2159464-just-one-cigarette-a-day-can-cause-serious-heart-problems/. Retrieved 6 May 2020.
- ↑ "Environmental tobacco smoke exposure and ischaemic heart disease: an evaluation of the evidence". BMJ 315 (7114): 973–80. 1997. doi:10.1136/bmj.315.7114.973. PMID 9365294.
- ↑ American Legacy Foundation factsheet on lung cancer ; their cited source is: CDC (Centers for Disease Control) The Health Consequences of Smoking: A Report of the Surgeon General. 2004.
- ↑ "Risk factors for acute myocardial infarction in Copenhagen. I: Hereditary, educational and socioeconomic factors. Copenhagen City Heart Study". Eur Heart J 10 (10): 910–16. 1989. doi:10.1093/oxfordjournals.eurheartj.a059401. PMID 2598948.
- ↑ Devereux G (2006). "ABC of chronic obstructive pulmonary disease. Definition, epidemiology, and risk factors". BMJ 332 (7550): 1142–44. doi:10.1136/bmj.332.7550.1142. PMID 16690673.
- ↑ "Exposures to environmental toxicants and attention deficit hyperactivity disorder in U.S. children". Environ. Health Perspect. 114 (12): 1904–09. 2006. doi:10.1289/ehp.10274. PMID 17185283.
- ↑ Tomar, S. L.; Asma, S. (May 2000). "Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey". Journal of Periodontology 71 (5): 743–51. doi:10.1902/jop.2000.71.5.743. ISSN 0022-3492. PMID 10872955.
- ↑ 19.0 19.1 Ramon, Jose-Maria; Echeverria, Jose-Javier (August 2002). "Effects of smoking on periodontal tissues". Journal of Clinical Periodontology 29 (8): 771–76. doi:10.1034/j.1600-051x.2002.290815.x. ISSN 0303-6979. PMID 12390575.
- ↑ Grossi, S.G.; Genco, R.J.; Machtet, E.E.; Ho, A.W.; Koch, G.; Dunford, R.; Zambon, J.J.; Hausmann, E. (1995). "Assessment of Risk for Periodontal Disease. II. Risk Indicators for Alveolar Bone Loss" (in en). Journal of Periodontology 66 (1): 23–29. doi:10.1902/jop.1995.66.1.23. ISSN 0022-3492. PMID 7891246. https://aap.onlinelibrary.wiley.com/doi/10.1902/jop.1995.66.1.23.
- ↑ Harris, C.; Warnakulasuriya, K.A.A.S.; Gelbier, S.; Johnson, N.W.; Peters, T.J. (December 1997). "Oral and Dental Health in Alcohol Misusing Patients". Alcoholism: Clinical and Experimental Research 21 (9): 1707–09. doi:10.1111/j.1530-0277.1997.tb04511.x. ISSN 0145-6008. PMID 9438534.
- ↑ Axeix, Tony; Hedin, C. Anders (December 1982). "Epidemiologic study of excessive oral melanin pigmentation with special reference to the influence of tobacco habits". European Journal of Oral Sciences 90 (6): 434–42. doi:10.1111/j.1600-0722.1982.tb00760.x. ISSN 0909-8836. PMID 6961509.
- ↑ Brocklehurst, Paul; Kujan, Omar; O'Malley, Lucy A; Ogden, Graham; Shepherd, Simon; Glenny, Anne-Marie (2013-11-19). "Screening programmes for the early detection and prevention of oral cancer". Cochrane Database of Systematic Reviews 2021 (11). doi:10.1002/14651858.CD004150.pub4. ISSN 1465-1858. PMID 24254989. PMC 8078625. https://www.cochrane.org/CD004150/ORAL_screening-programmes-for-the-early-detection-and-prevention-of-oral-cancer. Retrieved 9 May 2018.
- ↑ Monteiro-da-Silva, Filipa; Sampaio-Maia, Benedita; Pereira, Maria de Lurdes; Araujo, Ricardo (2013-03-04). "Characterization of the oral fungal microbiota in smokers and non-smokers". European Journal of Oral Sciences 121 (2): 132–35. doi:10.1111/eos.12030. ISSN 0909-8836. PMID 23489903.
- ↑ Reibel, Jesper (2003). "Tobacco and oral diseases. Update on the evidence, with recommendations". Medical Principles and Practice 12 (Suppl 1): 22–32. doi:10.1159/000069845. ISSN 1011-7571. PMID 12707498.
- ↑ Triggle, Nick (2017-07-01). "Pub smoking ban: 10 charts that show the impact" (in en-GB). BBC News. https://www.bbc.co.uk/news/health-40444460.
- ↑ "Tobacco 21". 2019-12-20. https://www.fda.gov/tobacco-products/retail-sales-tobacco-products/tobacco-21.
- ↑ "New WHO report pushes for stronger tobacco control policies" (in en). https://www.who.int/europe/news/item/04-07-2025-new-who-report-pushes-for-stronger-tobacco-control-policies.
- ↑ "Ban on cross-border tobacco advertising and sponsorship - Public Health" (in en). 2024-12-03. https://health.ec.europa.eu/tobacco/ban-cross-border-tobacco-advertising-and-sponsorship_en.
- ↑ Brones, Anna (2008-05-12). "Which country smokes the most?". http://www.gadling.com/2008/05/12/which-country-smokes-the-most/.
- ↑ "Cigarette Smoking Among Adults – United States, 2006". Cdc.gov. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5644a2.htm#fig.
- ↑ "Cigarette Smoking is a Risk Factor for Alzheimer's Disease: an Analysis Controlling for Tobacco Industry Affiliation". Journal of Alzheimer's Disease 19 (2): 465–80. 2010. doi:10.3233/JAD-2010-1240. PMID 20110594.
- ↑ "Effects of current and former cigarette smoking on the clinical course of Crohn's disease". Aliment. Pharmacol. Ther. 13 (11): 1403–11. 1999. doi:10.1046/j.1365-2036.1999.00630.x. PMID 10571595.
- ↑ "A meta-analysis of the role of smoking in inflammatory bowel disease". Dig. Dis. Sci. 34 (12): 1841–54. 1989. doi:10.1007/BF01536701. PMID 2598752.
- ↑ "Smoking in inflammatory bowel diseases: good, bad or ugly?". World J. Gastroenterol. 13 (46): 6134–39. 2007. doi:10.3748/wjg.13.6134. PMID 18069751.
- ↑ "Smoking and Diabetes" (in en-us). 23 April 2018. https://www.cdc.gov/tobacco/campaign/tips/diseases/diabetes.html.
- ↑ "Share of deaths from smoking". https://ourworldindata.org/grapher/share-deaths-smoking.
- ↑ Leslie Iverson, "Why do We Smoke?: The Physiology of Smoking" in Smoke, p. 318
- ↑ Leslie Iverson, "Why do We Smoke?: The Physiology of Smoking" in Smoke, pp. 320–21
- ↑ Varghese, J.; George, G.; Mathew, A. (2023). "A comprehensive review on the impacts of smoking on human health". Cureus 15 (10). doi:10.7759/cureus.46532. PMID 37900455. PMC 10625450. https://pmc.ncbi.nlm.nih.gov/articles/PMC10625450/.
- ↑ Model D (1985). "Smoker's face: an underrated clinical sign?". Br Med J (Clin Res Ed) 291 (6511): 1760–62. doi:10.1136/bmj.291.6511.1760. PMID 3936573.
- ↑ "Hazardous compounds in tobacco smoke". Int J Environ Res Public Health 8 (2): 613–28. 2011. doi:10.3390/ijerph8020613. PMID 21556207.
- ↑ "DNA damage responses: mechanisms and roles in human disease: 2007 G.H.A. Clowes Memorial Award Lecture". Mol. Cancer Res. 6 (4): 517–24. 2008. doi:10.1158/1541-7786.MCR-08-0020. PMID 18403632.
- ↑ "A novel application of the Margin of Exposure approach: segregation of tobacco smoke toxicants". Food Chem. Toxicol. 49 (11): 2921–33. 2011. doi:10.1016/j.fct.2011.07.019. PMID 21802474.
- ↑ "Mutagenicity of acrolein and acrolein-induced DNA adducts". Toxicol. Mech. Methods 20 (1): 36–44. 2010. doi:10.3109/15376510903530845. PMID 20158384.
- ↑ "Acrylonitrile-induced oxidative stress and oxidative DNA damage in male Sprague-Dawley rats". Toxicol. Sci. 111 (1): 64–71. 2009. doi:10.1093/toxsci/kfp133. PMID 19546159.
- ↑ "Epigenetic mechanisms of mouse interstrain variability in genotoxicity of the environmental toxicant 1,3-butadiene". Toxicol. Sci. 122 (2): 448–56. 2011. doi:10.1093/toxsci/kfr133. PMID 21602187.
- ↑ "[13C2-Acetaldehyde promotes unequivocal formation of 1,N2-propano-2'-deoxyguanosine in human cells"]. J. Am. Chem. Soc. 133 (24): 9140–43. 2011. doi:10.1021/ja2004686. PMID 21604744. https://figshare.com/articles/_sup_13_sup_C_sub_2_sub_Acetaldehyde_Promotes_Unequivocal_Formation_of_1_i_N_i_sup_2_sup_Propano_2_deoxyguanosine_in_Human_Cells/2639098. Retrieved 30 November 2019.
- ↑ "Mutagenicity of DNA adducts derived from ethylene oxide exposure in the pSP189 shuttle vector replicated in human Ad293 cells". Mutat. Res. 678 (2): 129–37. 2009. doi:10.1016/j.mrgentox.2009.05.011. PMID 19477295. Bibcode: 2009MRGTE.678..129T.
- ↑ "DNA-damaging ability of isoprene and isoprene mono-epoxide (EPOX I) in human cells evaluated with the comet assay". Mutat. Res. 629 (1): 7–13. 2007. doi:10.1016/j.mrgentox.2006.12.007. PMID 17317274. Bibcode: 2007MRGTE.629....7F.
- ↑ McCormack, VA.; Agudo, A.; Dahm, CC.; Overvad, K.; Olsen, A.; Tjonneland, A. et al. (November 2010). "Cigar and pipe smoking and cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC).". International Journal of Cancer 127 (10): 2402–2411. doi:10.1002/ijc.25252. PMID 20162568.
- ↑ Gay, Peter (1988). Freud: A Life for Our Time. New York: W.W. Norton & Company. pp. 650–51. ISBN 978-0-393-32861-5. https://archive.org/details/freudlifeforourt00gayp.
- ↑ Harris, J.R. (1998). The Nurture Assumption: Why children turn out the way they do. New York: Free Press.
- ↑ Parrott AC (1999). "Does cigarette smoking cause stress?". American Psychologist 54 (10): 817–20. doi:10.1037/0003-066X.54.10.817. PMID 10540594.
- ↑ Eysenck, H. J. (1965). Smoking, health and personality. New York: Basic Books.
- ↑ Ozga-Hess, Jenny E.; Romm, Katelyn F.; Felicione, Nicholas J.; Dino, Geri; Blank, Melissa D.; Turiano, Nicholas A. (2020-09-01). "Personality and impulsivity as predictors of tobacco use among emerging adults: A latent class analysis" (in en). Personality and Individual Differences 163. doi:10.1016/j.paid.2020.110076. ISSN 0191-8869. PMID 34321706.
- ↑ "Summaries for patients. Primary care interventions to prevent tobacco use in children and adolescents: U.S. Preventive Services Task Force recommendation statement". Ann. Intern. Med. 159 (8): 1–36. 2013. doi:10.7326/0003-4819-159-8-201310150-00699. PMID 23974179.
- ↑ Chamberlain, Catherine; O'Mara-Eves, Alison; Porter, Jessie; Coleman, Tim; Perlen, Susan M.; Thomas, James; McKenzie, Joanne E. (2017). "Psychosocial interventions for supporting women to stop smoking in pregnancy". The Cochrane Database of Systematic Reviews 2 (3). doi:10.1002/14651858.CD001055.pub5. ISSN 1469-493X. PMID 28196405.
- ↑ Stead, Lindsay F; Koilpillai, Priya; Fanshawe, Thomas R; Lancaster, Tim (2016-03-24). "Combined pharmacotherapy and behavioural interventions for smoking cessation". Cochrane Database of Systematic Reviews 2016 (3). doi:10.1002/14651858.cd008286.pub3. ISSN 1465-1858. PMID 27009521.
- ↑ "Featured Review: Can people stop smoking by cutting down the amount they smoke first?" (in en). https://www.cochrane.org/news/featured-review-can-people-stop-smoking-cutting-down-amount-they-smoke-first.
- ↑ "Average price of a pack of cigarettes". https://ourworldindata.org/grapher/average-price-of-a-pack-of-cigarettes.
- ↑ "Taxes as a share of cigarette price". https://ourworldindata.org/grapher/taxes-as-share-of-cigarette-price.
- ↑ "Enforcement of bans on tobacco advertising". https://ourworldindata.org/grapher/enforcement-of-bans-on-tobacco-advertising.
- ↑ "Support to help quit tobacco use". https://ourworldindata.org/grapher/support-to-help-to-quit-tobacco-use.
- ↑ "Share of people who smoke every day". https://ourworldindata.org/grapher/daily-smoking-prevalence-bounds.
- ↑ "Share of adults who smoke". https://ourworldindata.org/grapher/share-of-adults-who-smoke.
- ↑ "WHO global report on trends in prevalence of tobacco use 2000-2025, fourth edition" (in en). https://www.who.int/publications/i/item/9789240039322.
- ↑ Matthew Hilton, "Smoking and Sociability" in Smoke, p. 133
- ↑ See Gately; Wilbert
- ↑ Robicsek (1978), p. 30
- ↑ P. Ram Manohar, "Smoking and Ayurvedic Medicine in India" in Smoke, pp. 68–75
- ↑ González Wagner, Carlos (1984). Psicoactivos, misticismo y religión en el mundo antiguo. Complutense University of Madrid.
- ↑ Gilman & Xun 2004, pp. 20–21.
- ↑ Phillips, pp. 303–19
- ↑ Coe, pp. 74–81
- ↑ Jamestown, Virginia: An Overview
- ↑ Kulikoff, pp. 38–39.
- ↑ Cooper, William J., Liberty and Slavery: Southern Politics to 1860, Univ of South Carolina Press, 2001, p. 9.
- ↑ The People's Chronology, 1994 by James Trager
- ↑ 80.0 80.1 Lloyd & Mitchinson
- ↑ Tanya Pollard, "The Pleasures and Perils of Smoking in Early Modern England" in Smoke, p. 38
- ↑ 82.0 82.1 Timon Screech, "Tobacco in Edo Period Japan" in Smoke, pp. 92–99
- ↑ Gilman & Xun 2004, pp. 15–16.
- ↑ Roberts 2004, pp. 53–54.
- ↑ Burns, pp. 134–35.
- ↑ 86.0 86.1 86.2 Jos Ten Berge, "The Belle Epoque of Opium in Smoke, p. 114
- ↑ Stephen R. Platt, Imperial Twilight: the Opium War and the End of China's Last Golden Age (NY: Knopf, 2018), 166-73. ISBN 978-0-307-96173-0
- ↑ Benjamin Rush, M.D. (1798). Essays, Literary, Moral and Philosophical, 2nd ed. https://medicolegal.tripod.com/rush1798.htm. Retrieved 2 November 2019.
- ↑ James C. Coleman, Ph.D. (1976). Abnormal Psychology and Modern Life, 5th ed. Scott, Foresman & Co.. p. 43 and 427. OCLC 1602234.
- ↑ Proctor 2000, p. 178
- ↑ Proctor 2000, p. 219
- ↑ Proctor 2000, p. 187
- ↑ 93.0 93.1 Proctor 2000, p. 245
- ↑ Proctor, Robert N. (1996). Nazi Medicine and Public Health Policy. Dimensions, Anti-Defamation League. http://www.adl.org/Braun/dim_14_1_nazi_med.asp. Retrieved 2008-06-01.
- ↑ 95.0 95.1 Proctor 2000, p. 228
- ↑ White, Colin (September 1989). "Research on Smoking and Lung Cancer: A Landmark in the History of Chronic Disease Epidemiology". The Yale Journal of Biology and Medicine 63 (1): 29–46. PMID 2192501.
- ↑ Doll R, Hill AB; Hill (30 September 1950). "Smoking and carcinoma of the lung. Preliminary report". British Medical Journal 2 (4682): 739–48. doi:10.1136/bmj.2.4682.739. PMID 14772469.
- ↑ Doll R, Hill AB; Hill (26 June 1954). "The mortality of doctors in relation to their smoking habits. A preliminary report". British Medical Journal 1 (4877): 1451–55. doi:10.1136/bmj.1.4877.1451. PMID 13160495.
- ↑ Berridge, V. Marketing Health: Smoking and the Discourse of Public Health in Britain, 1945–2000, Oxford: Oxford University Press, 2007.
- ↑ "Smoking and Health: Report of the Advisory Committee to the Surgeon General of the Public Health Service". 1964. http://profiles.nlm.nih.gov/NN/B/B/M/Q/.
- ↑ "Reports of the Surgeon General, U.S. Public Health Service". http://www.surgeongeneral.gov/library/reports/.
- ↑ Geyelin, Milo (23 November 1998). "Forty-Six States Agree to Accept $206 Billion Tobacco Settlement". Wall Street Journal.
- ↑ VJ Rock; A Malarcher (2007-11-09). "Cigarette Smoking Among Adults – United States, 2006". United States Centers for Disease Control and Prevention. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5644a2.htm. "[...]In 2006, an estimated 20.8% (45.3 million) of U.S. adults[...]"
- ↑ Hilton, Matthew (2000-05-04). Smoking in British Popular Culture, 1800–2000: Perfect Pleasures. Manchester University Press. pp. 229–41. ISBN 978-0-7190-5257-6. https://books.google.com/books?id=UjM8t6Ul73YC&q=Smoking+in+British+Popular+Culture. Retrieved 2009-03-22.
- ↑ "WHO/WPRO-Smoking Statistics". World Health Organization Regional Office for the Western Pacific. 2002-05-28. http://www.wpro.who.int/media_centre/fact_sheets/fs_20020528.htm.
- ↑ Roberts 2004, pp. 46–57.
- ↑ WHO Report on the Global Tobacco Epidemic: The MPOWER Package (Report). Geneva. 2008. pp. 267–88. https://www.who.int/tobacco/mpower/2008/en/.
- ↑ History of the WHO Framework Convention on Tobacco Control.. Geneva: World Health Organization. 2009. ISBN 978-92-4-156392-5. OCLC 547193748.
- ↑ WHO Framework Convention on Tobacco Control.. Geneva, Switzerland: World Health Organization. 2003. ISBN 978-92-4-159101-0. OCLC 54966940.
- ↑ Chung-Hall, Janet; Craig, Lorraine; Gravely, Shannon; Sansone, Natalie; Fong, Geoffrey T. (2018-08-17). "Impact of the WHO FCTC over the first decade: a global evidence review prepared for the Impact Assessment Expert Group". Tobacco Control 28 (Suppl 2): tobaccocontrol–2018–054389. doi:10.1136/tobaccocontrol-2018-054389. ISSN 0964-4563. PMID 29880598.
- ↑ Republica. "Senior cardiologist Anil urges to quit smoking for the sake of loved ones" (in en). https://myrepublica.nagariknetwork.com/news/151296/.
- ↑ DoJ-DEA-History-1985-1990
- ↑ "Cracked up". 11 May 1999. http://www.salon.com/news/feature/1999/05/11/crack_media/index1.html.
- ↑ "Testosterone The good and the bad". CNN. Dec 1999. http://articles.cnn.com/1999-12-03/health/testosterone.wmd_1_testosterone-nanograms-risky-behavior.
- ↑ Robicsek (1978)
- ↑ Ashes to Ashes pp. 78–81
- ↑ Ivan Kalmar, "The Houkah in the Harem: On Smoking and Orientalist Art" in Smoke, pp. 218–29
- ↑ Greaves, p. 266
- ↑ Benno Tempel, "Symbol and File: Smoking in Art since the Seventeenth Century" in Smoke, pp. 206–17
- ↑ "Smoking in Film Noir Volume 1" (in en-GB). https://www.classicfilmnoir.com/p/smoking-in-film-noir.html.
- ↑ "Smoking Prevalence in UK Films | Doctor-4-U". https://www.doctor-4-u.co.uk/blog/2019/09/24/smoking-in-uk-films/.
- ↑ Noah Iserberg, "Cinematic Smoke: From Weimar to Hollywood" in Smoke, pp. 248–55
- ↑ 123.0 123.1 Thomas, Michael (2019). "Was Television Responsible for a New Generation of Smokers?" (in en). Journal of Consumer Research 46 (4): 689–707. doi:10.1093/jcr/ucz024.
- ↑ Tynan, Michael A.; Polansky, Jonathan R.; Driscoll, Danielle; Garcia, Claire; Stanton A. Glantz, PhD (2019). "Tobacco Use in Top-Grossing Movies — United States, 2010–2018" (in en-us). MMWR. Morbidity and Mortality Weekly Report 68 (43): 974–978. doi:10.15585/mmwr.mm6843a4. ISSN 0149-2195. PMID 31671080. PMC 6822812. https://www.cdc.gov/mmwr/volumes/68/wr/mm6843a4.htm.
- ↑ Fitzpatrick, Kevin (2019-07-05). "Netflix Will Curb Smoking Depictions After Stranger Things Complaint" (in en-US). Vanity Fair. https://www.vanityfair.com/hollywood/2019/07/stranger-things-netflix-smoking-complaint. Retrieved 2025-11-26.
- ↑ "New Truth Initiative report shows troubling use of tobacco imagery in TV shows, movies and music videos most popular among youth as e-cigarette epidemic persists". https://truthinitiative.org/sites/default/files/media/files/2022/10/Streaming%20press%20release_final_01.10.2022_1.pdf.
- ↑ Eugene Umberger, "In Praise of Lady Nicotine: A Bygone Era of Prose, Poetry... and Presentation" in Smoke, p. 241
- ↑ Eugene Umberger, "In Praise of Lady Nicotine: A Bygone Era of Prose, Poetry... and Presentation" in Smoke, pp. 236–47
- ↑ Willard A. Palmer Enlightening Thoughts of a Tobacco Smoker, in J. S. Bach: An Introduction to His Keyboard Music, p. 23. Accessed 2016.
- ↑ Stephen Cottrell, "Smoking and All That Jazz" in Smoke, pp. 154–59
- ↑ J. Edward Chamberlin & Barry Chevannes, "Ganja in Jamaica" in Smoke, p. 148
- ↑ J. Edward Chamberlin & Barry Chevannes, "Ganja in Jamaica" in Smoke, pp. 144–53
- ↑ Smith, Hilary. "The high costs of smoking". MSN money. Retrieved 10 September 2008 from https://web.archive.org/web/20081212025257/http://articles.moneycentral.msn.com/Insurance/InsureYourHealth/HighCostOfSmoking.aspx
- ↑ U.S. Department of Treasury. "The Economic Costs of Smoking in the United States and the Benefits of Comprehensive Tobacco Legislation". Retrieved 10 September 2008 from "Archived copy". http://www.treas.gov/press/releases/reports/tobacco.pdf.
- ↑ Sollmann, Torald. (1906) A Text-book of Pharmacology and Some Allied Sciences. W.B. Saunders Company, Philadelphia and London. p. 265.
- ↑ Matthew Hilton, "Smoking and Sociability" in Smoke, pp. 126–33
- ↑ "Health and Wellbeing - Smoking Reduction | Royal Navy" (in en). https://www.royalnavy.mod.uk/navyfit/health-and-wellbeing/smoking-reduction.html.
- ↑ Jahnke, Sara A.; Hoffman, Kevin M.; Haddock, C. Keith; Long, Mark A. D.; Williams, Larry N.; Lando, Harry A.; Poston, W. S. Carlos (2011). "Military tobacco policies: the good, the bad, and the ugly". Military Medicine 176 (12): 1382–1387. doi:10.7205/milmed-d-11-00164. ISSN 0026-4075. PMID 22338352. PMC 3282985. https://pmc.ncbi.nlm.nih.gov/articles/PMC3282985/.
- ↑ Skitt, Laura (2021-10-29). "What is the background to smoking in the military?" (in en). https://www.forcesnews.com/heritage/history/what-background-smoking-military.
- ↑ Smith, Elizabeth A.; Malone, Ruth E. (2014). "Mediatory myths in the U.S. military: tobacco use as "stress relief"". American journal of health promotion: AJHP 29 (2): 115–122. doi:10.4278/Ajhp.121009-QUAL-491. ISSN 2168-6602. PMID 24359178. PMC 4065229. https://pmc.ncbi.nlm.nih.gov/articles/PMC4065229/.
Further reading
- Ashes to Ashes: The History of Smoking and Health (1998) edited by S. Lock, L.A. Reynolds and E.M. Tansey 2nd ed. Rodopi. ISBN 90-420-0396-0
- Coe, Sophie D. (1994) America's first cuisines ISBN 0-292-71159-X
- Gately, Iain (2003) Tobacco: A Cultural History of How an Exotic Plant Seduced Civilization ISBN 0-8021-3960-4
- Goldberg, Ray (2005) Drugs Across the Spectrum. 5th ed. Thomson Brooks/Cole. ISBN 0-495-01345-5
- Goodman, Jordan, ed. Tobacco in History and Culture. An Encyclopedia (2 vol, Gage Cengage, 2005) online
- Greaves, Lorraine (2002) High Culture: Reflections on Addiction and Modernity. edited by Anna Alexander and Mark S. Roberts. State University of New York Press. ISBN 0-7914-5553-X
- Hirschfelder, Arlene B. Encyclopedia of smoking and tobacco (1999) online
- James I of England, A Counterblaste to Tobacco
- Lloyd, J & Mitchinson, J: "The Book of General Ignorance". Faber & Faber, 2006
- Marihuana and Medicine (1999), editor: Gabriel Nahas ISBN 0-89603-593-X
- Phillips J.E. (1983). "African Smoking and Pipes". The Journal of African History 24 (3): 3. doi:10.1017/s0021853700022039.
- Roberts, Allen F. (2004-08-15). "Smoking in Sub-Saharan Africa". in Gilman, Sander L.. Smoke: A Global History of Smoking. Reaktion Books. pp. 46–57. ISBN 978-1-86189-200-3. https://books.google.com/books?id=mM5bYb_uVcwC&q=smoke. Retrieved 2009-03-22.
- Robicsek, Francis (1978) The Smoking Gods: Tobacco in Maya Art, History, and Religion ISBN 0-8061-1511-4
- Gilman, Sander L.; Xun, Zhou (2004-08-15). "Introduction". in Gilman, Sander L.. Smoke: A Global History of Smoking. Reaktion Books. pp. 9–28. ISBN 978-1-86189-200-3. https://books.google.com/books?id=mM5bYb_uVcwC&q=smoke. Retrieved 2009-03-22.
- Wilbert, Johannes (1993) Tobacco and Shamanism in South America ISBN 0-300-05790-3
- Burns, Eric. The Smoke of the Gods: A Social History of Tobacco. Philadelphia: Temple University Press, 2007.
- Kulikoff, Allan. Tobacco & Slaves: The Development of Southern Cultures in the Chesapeake. North Carolina: University of North Carolina Press, 1986.
- Proctor, Robert N. (2000-11-15). The Nazi War on Cancer. Princeton University Press. ISBN 978-0-691-07051-3. https://books.google.com/books?id=02NGyKTwko0C&q=The+Nazi+War+on+Cancer. Retrieved 2009-03-22.
External links
| Wikivoyage has a travel guide for Smoking. |
- BBC Headroom - Smoking advice
- Cigarette Smoking and Cancer – National Cancer Institute
- Smoking & Tobacco Use – Centers for Disease Control
- Smoking – Our World in Data
- Treating Tobacco Use and Dependence – U.S. Department of Health and Human Services
- How to stop smoking – National Health Service UK
- NY Times: Responses to the targeting of teenage smokers
- Study ties more deaths, types of disease, to smoking (Feb 2015), Marilynn Marchione, Associated Press
-solution.jpg)





| Types |  | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Components | |||||||||||||
| Peripherals | |||||||||||||
| Culture | |||||||||||||
| Health issues | |||||||||||||
| Related products | |||||||||||||
| Tobacco industry | |||||||||||||
| Government and the law |
| ||||||||||||
| Lists | |||||||||||||
| |||||||||||||
 |  |
