Medicine:Chronic obstructive pulmonary disease
| Chronic obstructive pulmonary disease | |
|---|---|
| Other names | Chronic obstructive lung disease (COLD), chronic obstructive airway disease (COAD) |
 | |
| Section of a lung showing centrilobular emphysema, with enlarged airspaces in the centre of a lobule usually caused by smoking and a major feature of COPD | |
| Specialty | Pulmonology |
| Symptoms | Shortness of breath, chronic cough[1] Sputum production |
| Complications | Anxiety, depression, pulmonary heart disease, pneumothorax[2][1] |
| Usual onset | Over 35 years old[1] |
| Duration | Long term[1] |
| Causes | Tobacco smoking, air pollution, genetics[3] |
| Diagnostic method | Spirometry[4] |
| Differential diagnosis | Asthma, congestive heart failure, bronchiectasis, tuberculosis, obliterative bronchiolitis, diffuse panbronchiolitis[5] |
| Prevention | Stopping smoking, improving indoor and outdoor air quality, tobacco control measures,[3][6] occupational safety[7][8] |
| Treatment | Pulmonary rehabilitation, long-term oxygen therapy, lung volume reduction,[6] |
| Medication | Inhaled bronchodilators and steroids[6] |
| Frequency | 213 million (2021);[9] 2.7% of global population[9] |
| Deaths | 3.65 million (2021);[10] 5% of global deaths[3] |
Chronic obstructive pulmonary disease (COPD) is a long-term lung condition that makes it progressively harder to breathe. It occurs when the airways and lung tissue become damaged, leading to reduced airflow and less efficient oxygen exchange in the lungs. COPD develops gradually over time, and while it cannot currently be cured, treatments and lifestyle changes can help control symptoms and slow disease progression.[11][12] Early diagnosis and treatment are recommended.[7][13][14]
The condition includes two related lung problems: chronic bronchitis and emphysema. Chronic bronchitis involves ongoing inflammation of the airways, causing excess mucus production, coughing, and chest discomfort. Emphysema involves damage to the small air sacs in the lungs, which reduces the lungs' ability to transfer oxygen into the bloodstream. Many people with COPD experience shortness of breath, persistent cough, wheezing, and reduced exercise tolerance. Symptoms can become more severe during acute flare-ups, which can be triggered by bacterial and viral infections and exposure to irritants.[15] People with COPD generally display a combination of these symptoms, and are likely to have additional health issues.[13][16]
COPD can develop due to multiple factors, most often involving long-term exposure to lung irritants. The strongest risk factors are tobacco smoke, air pollution, and workplace dust and chemical fumes. Smoke from fuels used for cooking and heating is a major risk factor in some places, particularly for women and young children. Factors affecting lung development in early life such as respiratory infections, poor nutrition, and physical inactivity, can increase risk of COPD in later life.[17] Genetics can also play a role.
Diagnosis of COPD is usually confirmed using lung function tests that measure how well air moves in and out of the lungs. While COPD cannot currently be cured, treatment can significantly improve quality of life. Common treatments include inhaled medications that help open the airways, pulmonary rehabilitation programmes that improve fitness and breathing control, and oxygen therapy for people with advanced disease. Quitting smoking is strongly recommended, as is reducing exposure to other lung irritants.
As of 2021, COPD affected about 213 million people worldwide.[9] COPD typically occurs in people over the age of 35–40,[1] and risk increases with age.[11] In 2021, COPD was the fourth-biggest cause of death, responsible for approximately 5% of total deaths.[3] Almost 90% of COPD deaths in those under 70 years of age occur in low and middle income countries.[3] The number of deaths is projected to increase further because of continued exposure to risk factors and an ageing population.[11]
Signs and symptoms

The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines COPD as a lung condition with multiple underlying causes, characterized by long-lasting respiratory symptoms (shortness of breath, cough, and mucus) which can flare up intermittently. Symptoms are due to impairments of the airways (bronchitis, bronchiolitis) or small air sacs of the lungs (emphysema) that cause persistent, often progressive, airflow obstruction.[18][19][20]
Shortness of breath
A cardinal symptom of COPD is chronic and progressive shortness of breath. Breathlessness is often the most distressing symptom, causing anxiety and the level of disability that is experienced.[4] Symptoms of wheezing and chest tightness associated with breathlessness can vary over the course of a day or between days and are not always present. Chest tightness often follows exertion.[4]
People experiencing distress may naturally adopt a sitting posture, leaning forward with their hands on their knees, known as the tripod position. This can help to decrease breathlessness by stabilizing and lifting the shoulder girdle.[21] People with more advanced COPD may also breathe through pursed lips, which can improve shortness of breath.[22]
Shortness of breath often results in reduced physical activity, and low levels of physical activity are associated with worse outcomes.[23][24] People with COPD often have increased breathlessness and frequent colds before seeking treatment. In severe and very severe cases there may be constant tiredness, weight loss, muscle loss and anorexia.[4]
Cough
The first symptom of COPD to appear is usually a chronic cough, which may or may not bring up thick slippery fluid (referred to as sputum, mucus or phlegm). Coughing up of mucus can be intermittent and may be difficult to evaluate. A productive cough that brings up mucus is seen in less than 30% of cases. Sometimes, limited airflow may develop in the absence of a cough. Symptoms are usually worse in the morning.[25] Depending on social or cultural factors, mucus may be swallowed or spat out.[4]
A chronic productive cough may result from the release of too much mucus within airways. When it persists for more than three months each year for at least two years, it is called chronic bronchitis.[26] Chronic bronchitis can occur before the restricted airflow diagnostic of COPD.[11] People tend to under-report symptoms, and may assume that symptoms result from short-term irritation rather than underlying changes in lung function.[11] In severe COPD, vigorous coughing may lead to rib fractures or to a brief loss of consciousness.[4]
Exacerbations
An acute exacerbation is a sudden flare-up or worsening of signs and symptoms that lasts from several days[27] to two weeks.[28] Worsening of symptoms can involve increased breathlessness, increase in mucus volume, change in mucus character, or change in cough or wheeze.[27][28] A commonly found sign is air trapping, difficulty in breathing out fully.[29]
Flare-ups are often associated with inflammation resulting from viral or bacterial infection or environmental irritation of the airways. Viral infections such as the common cold account for 70% of flare-ups.[26] Colds more often occur during the winter months but can occur at any time.[30] Bacterial respiratory infections are the second most frequent triggers, including Haemophilus influenzae,[31][28] Pseudomonas aeruginosa[32][28] and Streptococcus pneumoniae.[28] Bacterial infections may occur in combination or be secondary to viral infections.[33]
Environmental insults that can trigger acute flare-ups include exposure to smoking, use of solid fuels, and other sources of indoor or outdoor air pollution.[28] Exposure to tobacco smoke can be either active or passive.[34] Smoke from wildfires is an increasing risk in many parts of the world due to climate change.[35] Government agencies have published protective advice on their websites. In the US the EPA recommends the use of well-fitting particulate masks, which give more effective protection than dust masks when dealing with the fine particles from wildfires.[36] This same advice is offered in Canada and Australia regarding forest fires.[37][38]
The risk of developing a COPD flare-up is higher in women; in people with one or more flare-ups in the last year; in those with more severe COPD as measured by lung function tests; and in those with chronic bronchitis or related conditions such as gastroesophageal reflux, pulmonary hypertension[28] or pulmonary embolism.[39] People with two or more flare-ups a year are associated with worse disease progression and are classed as frequent exacerbators.[29] More flare-ups are associated with more rapid decline in lung function, lower quality of life, and higher morbidity and mortality.[28] Frailty in ageing is linked to more flare-ups and hospitalizations.[40]
Other conditions
COPD often occurs along with multiple other conditions (comorbidities) affecting the body's systems. This reflects both shared risk factors and the role of inflammation as a mechanism by which illness develops.[16] Compared to people of the same age without COPD, people with COPD have higher rates of cardiovascular disease, respiratory conditions (lung cancer, pneumonia and asthma), musculoskeletal conditions (osteoporosis), neuropsychiatric conditions (depression, dementia,[13] anxiety[41][2][1]), and metabolic disorders (diabetes mellitus,[41] metabolic syndrome, chronic kidney disease,[42] and skeletal muscle dysfunction).[16][43] Cognitive impairment is common in those with COPD, as it is for other lung conditions that affect airflow. Cognitive impairment is associated with the declining ability to cope with the basic activities of daily living.[44]
People with COPD have up to 83% higher risk of pneumonia, atrial fibrillation, and heart failure, and 78% higher risk of depression.[13] Metabolic syndrome has been seen to affect up to 50% percent of those with COPD and significantly affects the outcomes.[45] When metabolic syndrome occurs with COPD, there is more systemic inflammation.[45] Metabolic syndrome on its own has a high rate of morbidity and mortality, and this rate is amplified when it occurs with COPD.[26]
There is also an associated risk of developing pulmonary hypertension, lead to worse outcomes, including the risk of death.[46] The likelihood that pulmonary hypertension will complicate COPD has been reported as 39%.[46] Of the people with COPD listed for lung transplantation, 82% were documented as having pulmonary hypertension.[46]
Other complications include reduced quality of life and increased disability, cor pulmonale, chest infections, secondary polycythemia, respiratory failure, pneumothorax, and cachexia (muscle wasting).[1][2][47] Tuberculosis is a risk factor for the development of COPD, and is also a potential comorbidity.[26][8]
In cases of COVID-19, COPD patients were at higher risk for severe complications, including hospitalization, intensive care unit admission, and mortality. They were also likely to display symptoms of Long COVID involving persistent respiratory symptoms, fatigue, and cognitive dysfunction.[48] Differentiating COVID-19 symptoms from an exacerbation is difficult; where symptoms include loss of taste or smell, COVID-19 is to be suspected.[49]
People with COPD have more additional health issues than those without COPD.[13] Multimorbidity is associated with a worse COPD prognosis.[16] People with COPD are more likely to die of respiratory or heart-related causes than those without COPD, and to die at younger ages.[13] People with COPD often die as a result of comorbidities rather than from respiratory problems.[50]
Categorization
Categorizing COPD in terms of subtypes can support more targeted treatment approaches for patients.[51][12] A phenotype refers to a collection of observable characteristics including symptoms, frequency of episodes, and other details of patient history that are used in clinical practice. An endotype links such observable traits to underlying mechanisms. One phenotype may be related to multiple endotypes.[12] A genotype is based on the presence or absence of a genetic factor and its effects on underlying mechanisms.[52] An etiotype is a grouping based on contributory causes. Individuals can be affected by multiple causes. Specific causes may be related to particular phenotypes.[12]
Emphysema and chronic bronchitis phenotypes
Historically, phenotypic definitions of COPD have often focused on symptoms of emphysema and chronic bronchitis.[12] Emphysema involves enlarged air sacs in the lungs (alveoli) whose walls break down resulting in permanent damage to the lung tissue. Emphysema can exist without airflow limitation, but commonly involves it. Other structural abnormalities can also limit airflow.[53] Chronic bronchitis is defined as a productive cough that is present for at least three months each year for two years. It does not always result in airflow limitation, although the risk of developing COPD is great.[26]
Early categorizations grouped patients on the basis of physical symptoms as type A and type B. Type A (emphysema types) were known as pink puffers due to their pink complexion, fast breathing rate and pursed lips. Type B (chronic bronchitic types) were referred to as blue bloaters due to low oxygen levels causing a bluish color to the skin and lips and swollen ankles.[54][55] Recently, it has been suggested that these early phenotypes may reflect unique underlying mechanisms: an "emphysematous phenotype" that involves destruction of air sacs (alveoli) and a "chronic bronchitis phenotype" associated with airway inflammation.[12][56] Most people with COPD have a combination of symptoms reflecting both emphysema and airway disease.[54]
Other phenotypes
COPD is complex, and is increasingly recognized as a diverse group of disorders with differing risk factors and clinical courses. This has resulted in other subtypes or phenotypes of COPD being proposed.[57][58] A common phenotype is the frequent exacerbator, someone who has had two or more flare-ups within a year. Frequent exacerbators have a poor prognosis, so identifying them and preventing further flare-ups is a major concern.[29][56]
Asthma-COPD overlap (ACO phenotype), a condition with clinical features of both asthma and COPD, is another proposed subtype of COPD. It is considered by some to be a separate medical condition.[59][12] A pulmonary vascular COPD phenotype has been described involving cardiovascular dysfunction.[60] A molecular phenotype of CFTR dysfunction is shared with cystic fibrosis.[61] A combined phenotype of chronic bronchitis and bronchiectasis has been described, with a difficulty noted in determining the best treatment.[62] The identification and recognition of different phenotypes can guide appropriate treatment approaches.[63]
Genotypes
The alpha-1 antitrypsin deficiency (AATD) genetic subtype involves a rare mutation in the SERPINA1 gene that is linked to proteinase-antiprotease imbalance. In this genotype, unchecked activity of elastase in white blood cells called neutrophils leads to early-onset emphysema. A treatment for this type of COPD has been proposed, involving intravenous administration of purified AAT protein.[12][52][19]
Endotypes
An endotype is defined in terms of a biological or molecular mechanism that explains why a given patient has specific observable disease features.[12][41] Two well-defined COPD endotypes are related to inflammation mechanisms of white blood cells in the immune system. The types of white blood cells involved are neutrophils and eosinophils.[12]
Neutrophils are a type of white blood cell that deals with injury and infection. Environmental stressors (e.g. cigarette smoke, air pollution) cause inflammation of neutrophils in airways, resulting in release of interleukin (IL)−1, IL-8, Th17 and other chemical messengers. This is called the neutrophil-centric inflammasome pathway, or "T2-low" COPD. Patients display elevated levels of IL-17 and other proteins related to neutrophils. Their symptoms align with the classical smoking-associated chronic bronchitis phenotype. This endotype is associated with accelerated decline in lung function and recurrent infectious flare-ups.[12][41]
Eosinophils are white blood cells involved in allergies and asthma. Mechanisms involved are similar to those in allergen response, and similar, but not identical, to those in asthma. In a pathway known as IgE-independent mast cell activation, mast cells release inflammatory chemical messengers (histamine and tryptase), stimulatingType 2 helper cells to produce cytokines (IL-4, IL-5, and IL-13). This drives inflammation of eosinophils and mucus production. This is called eosinophil-dependent type 2 immunity or "T2-high" COPD. 20–40% of COPD patients display activation of type 2 immune pathways with elevated eosinophil counts in blood or sputum. They have "asthma-like" symptoms, and higher risk of flare-ups and hospitalization. The "T2-high" endotype may overlap with the ACO phenotype.[12][64][41]
Etiotypes
In 2023, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) recognized the variety of causes contributing to COPD by introducing a new classification system categorizing COPD in terms of underlying causes and risk factors, or etiotypes. The 2023 GOLD report identifies seven distinct etiotypes:[12][18]
- cigarette smoking COPD (COPD-C)
- biomass and pollution exposure COPD (COPD-P)
- genetically determined COPD (COPD-G)
- COPD due to abnormal lung development (COPD-D)
- COPD with asthma (COPD-A)
- COPD due to infections (COPD-I)
- COPD of unknown cause (COPD-U)
This framework better reflects variation in COPD causes and disease progression in global populations. In low-and middle-income countries, COPD related to the burning of organic materials as fuels (COPD-P) and to repeated childhood respiratory infections (COPD-I) are more common.[12]
Identification of causes has implications for disease management. Some etiotypes can be related to specific clinical phenotypes. For example, biomass and pollution-associated COPD (COPD-P) tends to involve greater tissue damage to small airways and obstruction of airflow, while tobacco-related disease (COPD-C) involves more damage to air sacs and reduces oxygen transfer to the bloodstream.[12] Identification of such differences emphasizes the need to address underlying issues. Health programs to improve early-life lung development can be part of COPD prevention and management. Providing clean energy cooking fuels can reduce biomass exposure. Vaccination can help to prevent respiratory infections such as influenza, pneumococcus, and RSV, and reduce dangerous COPD flare-ups.[12]
Causes
COPD tends to develop as a result of exposure to harmful particles or gases, including tobacco smoke, that irritate the lung. This causes significant or long-term inflammation that interacts with individual host factors.[11] The greatest risk factor for the development of COPD is tobacco smoke,[66] accounting for up to 70% of cases in first-world countries.[41] Exposure can be either active (smoking yourself) or passive (living in a house where someone else smokes).[17]
Up to 30% of COPD cases occur in people who have never smoked, and many heavy smokers do not develop COPD, so other factors also need to be considered.[17][67] These include exposure to indoor and outdoor pollutants, particulate matter, allergens, occupational exposure, and host factors.[25][26] In developing countries, poorly ventilated cooking and heating fires are a common cause of COPD, particularly for women and young children.[26] COPD is also caused by exposure to occupational irritants[7] such as dust from farming (e.g. grains), manufacturing (e.g. cadmium dust or fumes), mining,[68] and construction. The three main types of construction dust are silica dust, non-silica dust (e.g., dust from gypsum, cement, limestone, marble and dolomite) and wood dust.[69]
Host factors include genetic susceptibility.[26] Alpha-1 antitrypsin deficiency (A1AD) is an important genetic risk factor for COPD.[70] It is advised that everybody with COPD be screened for A1AD.[43]
Other host factors are associated with poverty,[71] physical inactivity and ageing.[26] The role of changes in lung function throughout life is increasingly being recognized in COPD. Early-life factors can contribute to abnormal lung development and increase the risk of COPD in later life. Many early-life risk factors could be prevented, such as poor nutrition, low physical activity, early alcohol consumption, and exposure to smoking and biomass fumes.[17] Another host factor that can arise during development is airway branching variation.[72] In Europe, airway hyperresponsiveness is rated as the second most important risk factor after smoking.[26] It can contribute to asthma, which is recognized as an additional risk factor.[26]
Alcohol abuse can lead to alcoholic lung disease and is seen to be an independent risk factor for COPD.[73][74] Mucociliary clearance is disrupted by chronic exposure to alcohol; macrophage activity is diminished and an inflammatory response promoted.[75][76] The damage leads to a susceptibility for infection, including COVID-19,[77] which is increased when combined with smoking. Smoking induces the upregulation of the expression of ACE2, a receptor for the SARS-CoV-2 virus.[73]
Smoking
The greatest risk factor for the development of COPD globally is tobacco smoking.[66][41] Exposure can be either active (smoking yourself) or passive (living in a house where someone else smokes).[17] The second most frequent substance that is smoked is marijuana. Although marijuana smoking carries a lower risk for COPD than tobacco smoking, chronic marijuana smoking is still associated with increased respiratory symptoms similar to those of chronic bronchitis.[78] The highest level of risk is associated with smoking both marijuana and tobacco. This carries a higher symptom burden and greater risk of developing COPD compared to smoking tobacco only or to marijuana only.[78] Vaping is also associated with an increased risk of COPD.[79][80]
Tobacco
Smokers and ex-smokers have a higher rate of developing COPD.[11][66] In high-income countries smoking is associated with over 70% of COPD cases, while in low and middle income countries, it accounts for 30% to 40% of cases.[41] In the United States and United Kingdom, of those with COPD, 80–95% are either current or previous smokers.[81][82][83] About 20% of those who smoke will develop COPD,[81] and about 50% of heavy smokers will get COPD.[11]
Several studies indicate that women are more susceptible than men to the harmful effects of tobacco smoke.[84] Given the same amount of cigarette smoking, women have a higher risk of COPD than men.[85] Women who smoke during pregnancy, and during the early life of their child, also increase risk of their child's later development of COPD.[86] Epigenetic studies support this link, showing that ACSF3 is differentially methylated in smoke-exposed fetal lungs, and an integrative study identified it as a key regulator of COPD.[87]
Inhaled smoke triggers the excessive release of proteases. This degrades elastin, the major component of the walls of alveoli, the small air sacs in the lungs. Damage to the cell walls interferes with their ability to transfer oxygen from the lungs to the bloodstream.[66] Smoke also interferes with cilia, limiting their ability to clear mucus, cellular debris and unwanted fluid from airways in the respiratory tract.[66]
Other methods of inhaling tobacco smoke, such as cigar, pipe, water-pipe and hookah use, also confer a risk.[26] Water-pipe or hookah smoke appears to be as harmful or even more harmful than smoking cigarettes.[88]
Marijuana
Marijuana is the second most commonly smoked substance.[89] Both cannabis and tobacco smoke contain toxic and carcinogenic compounds such as polycyclic aromatic hydrocarbons (PAHs), volatile organic compounds (VOCs) and reactive oxygen species (ROS). These cause DNA, cell and tissue damage through mechanisms of oxidative stress and chronic inflammation which are involved in COPD. However, there are differences in the effects of marijuana and tobacco use.[78]
Tobacco smoke has a bronchoconstrictive effect that tightens smooth muscle in the lungs, contributing to coughing, wheezing, and tightness in the chest. In contrast, marijuana use has a bronchodilatory effect that can temporarily counteract airflow obstruction. At lower levels (a few joints per month) cannabis smoking may not cause the type of structural damage in small airways that occurs in tobacco smoking, and leads to airflow limitation and severe shortness of breath.[78]
In contrast, heavier and prolonged cannabis use (>20 uses per month) leads to chronic inflammation and impaired function in large airways, likely due to the effects of PAHs and VOCs.[78] Chronic cannabis use is associated with increased respiratory symptoms similar to those in chronic bronchitis, including cough, mucus production and wheezing. One study reported that damaging effects on large airway function of a single cannabis joint were comparable to 2.5 to 5 tobacco cigarettes.[78] Also, marijuana smokers typically reported onset of respiratory symptoms ten years earlier than tobacco smokers.[89] There is evidence that some cannabis-related respiratory symptoms appear to resolve if users stop smoking, whereas tobacco smokers continue to decline despite stopping.[89]
Combined tobacco and marijuana use
However, when someone smokes both marijuana and tobacco, either in combination or separately, their risk increases more highly, a synergistic effect. Those who smoke both tobacco and cannabis show a higher symptom burden and COPD risk than those who smoke only tobacco (known to affect both large and small airways), or only marijuana (known to affect large airway function). The increase in risk was particularly noticeable at high levels of cumulative cannabis exposure (>50 joints lifetime).[78] Using both marijuana and tobacco appears to have a cumulative toxic effect, and may increase risk for conditions such as bullous emphysema,[90] spontaneous pneumothorax, and lung cancer.[78][91][89][92]
Pollution

Air pollution is a major cause of COPD, contributing an estimated 50% of the total attributable risk of COPD worldwide.[94] It is the leading known risk factor for COPD in life-long nonsmokers,[94] and has no safe threshold.[65] Air can contain a mix of potentially harmful suspended particles and chemicals such as carbon monoxide, heavy metals, lead, ozone, nitrogen oxides (NOx), sulfur oxides, polycyclic aromatic hydrocarbons, benzene and acrolein. Both particulate matter and gases in air pollution contribute to COPD pathophysiology.[94][95][96][7]
The harmfulness of particulate matter depends on the size, structure and composition of the particles involved. Particulate matter can carry toxic metals and organic matter and transport them through the lower and upper respiratory tracts deep into the lungs.[94][95] Exposure to particulates can contribute to the development of COPD and trigger flare-ups either directly through irritation or indirectly due to infections.[45]
Air pollution is often described in terms of ambient (outdoor) and household (indoor) air pollutants.[94] Major sources of ambient air pollution include suspended dusts, combustion of fossil fuels and biofuels, industrial emissions,[94][95] waste disposal,[97] and wildfire smoke. Combustion releases fine and ultrafine particulates, greenhouse gases and other pollutants. Photochemical reactions between sunlight, nitrogen oxides (NOx) and volatile organic compounds (VOCs) produce ozone,[94] which increases the risk of death from COPD.[95] Black carbon or soot is an air pollutant associated with an increased risk of hospitalization from flare-ups. Long-term exposure brings with it an increased rate of mortality.[45][95]
The main indoor air pollutants include particulate matter, VOCs, nitrogen oxides, sulfur dioxide, carbon monoxide, ozone, radon, toxic metals, and microorganisms.[98] Smoking is a major contributor to indoor air pollution, as is the burning of wood and other biomass fuels for heating and cooking. Building materials and furnishings can be sources of formaldehyde, asbestos, and lead dust. Chemicals in cleaning products, paints, varnishes, pesticides, fragrances, air fresheners, and office equipment can release VOCs and aerosols. Microorganisms include mold, fungi, bacteria, and dust mites.[98] Workplace-related exposures in occupations such as farming, cleaning and industrial work[99] include dust from grinding, blasting, and sanding,[7] grain dust,[99] cleaning solutions and pesticides.[100] Radon gas occurs naturally and can enter buildings through cracks in foundations and walls. Pollutants from outdoor air can also enter buildings.[98]
Comparisons of COPD rates between cities and rural areas can vary widely and tend to reflect underlying factors such as gender, smoking (rural people may smoke more), work-related pollutant exposure (grain dust and pesticides in rural areas, manufacturing in cities), and accessibility to health care.[101][102][103] Areas with poor outdoor air quality, including that from exhaust gas, generally have higher rates of COPD.[104] 97% of the major cities in the world fail to meet the World Health Organization (WHO)'s safety standards for particulate matter in ambient air.[94] Urban air pollution significantly affects the developing lung and its maturation, and is a potential risk factor for the later development of COPD.[26]
Patients with COPD in rural areas experience greater morbidity and obstacles to care than those in urban areas. Racial/ethnic minorities and those with low incomes, particularly in rural areas, are also at greater risk of forgoing doctor visits due to cost.[102]
Measures to prevent and control air pollution and reduce emissions have been taken by some governments, and have significantly reduced both pollution and COPD incidence. When pollution levels outdoors are high, people can reduce risk by wearing personal protective equipment such as an N95 mask, and by reducing the time and intensity of outdoor activities. Quitting smoking, using clean fuels for heating and cooking, and improving ventilation are important steps for improving indoor air quality and reducing COPD risk.[95]
Biomass fuels
Between 2 and 3 billion people (most of whom are in low-income countries) cook, heat or light their homes using solid biomass fuels such as wood, crop wastes, charcoal, or dry dung.[105][106] Poorly ventilated open fires and simple stoves used for cooking and heating often use biomass fuels, kerosene, or coal, generating very high levels of indoor air pollution.[26][105] Globally, 50% of all households and 90% of rural households are estimated to use such fuels.[105] They are the main source of energy in 80% of homes in India, China and sub-Saharan Africa.[104] Wood is also used for household heating in developed countries (e.g. Canada, Australia, USA), but there, use tends to be seasonal and involve lower exposure levels.[105]
Use of biomass fuels increases indoor air pollution and is one of the most common causes of COPD in developing countries. Women tend to do the work of cooking and other tasks at home. This increases women's exposure to indoor pollutants and the level to which they are affected.[26] Small children who tend to be at home, and whose lungs are still developing, are also likely to be more affected.[107] Exposure to indoor biomass smoke has been associated with acute lower respiratory infections in children younger than five, and with COPD in men and women age 30 or more. The overall risk of COPD for indoor biomass exposure was estimated at 3.2 for women and 1.8 for men.[105]
Improving cookstoves and kitchen ventilation, and using clean fuels for heating and cooking, are important steps for reducing indoor COPD risk. Changing from biomass fuel to biogas when cooking has been shown to reduce COPD risk. Improving conditions for longer periods of time more effectively countered decline in lung function.[95][95]
Occupational exposure
Exposure to workplace dusts, chemicals and fumes in a wide variety of industries increases the risk of COPD in smokers, nonsmokers[99][7][108] and never-smokers.[109][8][108] In the United States, workplace exposure is estimated to be the cause of COPD in 31.1% of cases in never-smokers and 19.2% of all cases. Workplace exposure probably represents a greater risk in countries with insufficient regulations.[26] In China, the highest occupational risks were associated with agriculture (farming, forestry, animal husbandry, and fishery), followed by manufacturing and mining. Exposure level (low, medium or high) correlated with severity of COPD.[68]
Substances implicated in occupational exposure include organic dusts[99] (e.g. dusts from grains, flour, paper- and textile-making), inorganic dusts (e.g. cadmium, silica, coal dust, asbestos, cement), fumes from cadmium and welding,[7][110][26] and irritant gases used in industrial production and in cleaning (e.g. nitrous fumes, sulphur dioxide and chlorine).[26]
The negative effects of occupational exposure and smoking are interrelated and the two factors may be additive or synergisticly reinforce each other.[7] Symptoms differ. Compared to smokers with COPD, never-smoking patients with COPD are more likely to have symptoms of asthma and bronchiectasis, and a history of pulmonary tuberculosis, and less likely to have symptoms of emphysema.[8]
Occupational exposures may be under-diagnosed, particularly in never-smokers. Taking a detailed occupational history and identifying possible occupational causes is important for intervention and management of COPD. Exposure to dusts and gases in the workplace is potentially reduceable through regulation, education and training, and increased use of safety measures and protective equipment.[7][8]
Genetics
Genetics plays a role in the development of COPD. COPD is more common among relatives of those with COPD who smoke than among unrelated smokers.[26] The most well known genetic risk factor is alpha-1 antitrypsin deficiency (AATD) and this is the only genotype (genetic subtype) with a specific treatment.[52] This risk is particularly high if someone deficient in alpha-1 antitrypsin (AAT) also smokes.[111] It is responsible for about 1–5% of cases[111][112] and the condition is present in about three to four in 10,000 people.[113]
Mutations in MMP1 gene that encodes for interstitial collagenase are associated with COPD.[114]
The COPDGene study is an ongoing longitudinal study into the epidemiology of COPD, identifying phenotypes and looking for their likely association with susceptible genes. Genome-wide analyses in concert with the International COPD Genetics Consortium has identified more than 80 genome regions associated with COPD. Whole genome sequencing is an ongoing collaboration (2019) with the National Heart, Lung and Blood Institute (NHLBI) to identify rare genetic determinants.[115]
Abnormal lung development
The role of lung function throughout life is increasingly being recognized.[17] It has been suggested that having smaller airways relative to lung size is a possible indicator of whether someone is likely to develop COPD.[116] Mechanisms such as abnormal lung development and accelerated lung function decline, beginning early in life, can lead to COPD in late adulthood. Some early-life factors that contribute to poor lung development may be preventable, such as poor nutrition, low physical activity, early alcohol consumption, and exposure to smoking.[17]
A host factor of an airway branching variation, arising during development, has been described.[72] A branch variant in the central airway is specifically associated with an increased susceptibility for the later development of COPD. A genetic association for the variants with FGF10 has been suggested.[72][117]
In Europe, airway hyperresponsiveness (AHR) is rated as the second most important risk factor after smoking.[26] In AHR, smooth muscle in airways becomes more sensitive. It is more likely to tighten in response to stimuli in the environment (direct AHR), or chemical messengers released by mast cells (indirect AHR). This drives eosinophilic and type 2 helper T lymphocyte-driven airway inflammation. It may lead to airway structural changes known as remodeling and airflow obstruction. In those with asthma, AHR can contribute to breathlessness, wheeze, and chest tightness.[118] AHR may be a treatable trait.[119][120]
Asthma
A history of asthma in childhood is associated with decreases in adult lung function and higher susceptibility to COPD.[121][122] Asthma is a recognized risk factor: the comorbidity of COPD is reported to be 12 times higher in patients with asthma after adjusting for smoking history.[26] Asthma commonly starts in childhood, with variable symptoms of breathlessness, chest tightness, cough and wheeze. Appearance of symptoms may relate to times of day and to identifiable triggers such as dust, pollen, and grass.[123] In contrast, COPD has a later onset and is progressive; airflow limitation in COPD is poorly reversible; and respiratory symptoms in COPD are persistent.[124]
Asthma predominantly involves eosinophilic and type 2 helper T lymphocyte-driven airway inflammation.[123] It has been suggested that a diagnosis of asthma in childhood may be associated with poor lung function in adulthood.[17] The occurrence of both asthma and COPD, referred to as Asthma-COPD overlap (ACO), is associated with increased severity of respiratory symptoms, increased hospital admission, and worse quality of life, compared to either asthma or COPD alone[124] Asthma patients who have been exposed to higher levels of air pollution are observed to be almost three times more likely to develop ACO.[95] Higher incidence of ACO is related to specific industries and occupations, indicating the importance of workplace exposures on respiratory health.[124]
Infections
A history of respiratory infections in childhood is associated with decreases in adult lung function and higher susceptibility to COPD.[121][125] Both tuberculosis and pneumonia in childhood are risk factors for COPD, with adult COPD patients experiencing worse symptoms and poorer lung function as measured by spirometry.[126][8]
COPD and non-COPD patients tend to experience different types of infections. COPD patients are more likely to report infections from gram-negative bacteria (Pseudomonas aeruginosa, Haemophilus influenzae) and fungal pathogens.[32]
Pathophysiology

COPD is a progressive lung disease characterized by narrowed airways, which prevent air from moving freely; excess mucus, which clogs air passages; and breakdown of lung tissue in small air sacs, which then fail to transfer oxygen into the bloodstream efficiently. Poor airflow due to lung damage (airflow limitation) tends to be chronic and incompletely reversible. Small airway disease (SAD) is the main driver of airflow limitation, through mechanisms of narrowing, chronic inflammation, and airway remodeling,[127] while emphysema destroys air sacs and limits the transfer of oxygen.[128] Those with COPD may have difficulty in breathing out fully (air trapping). If air cannot fully escape the lungs, the lungs may expand past their normal size (hyperinflation), increasing breathing difficulty.[129][130]
The relative contributions of small airway disease and emphysema vary from person to person.[11] There are sex differences in the anatomy of the respiratory system between men and women. Women tend to have smaller airway lumens and thicker airway walls, which may contribute to increased severity of COPD symptoms and frequency of COPD flare-ups for women.[131]
COPD develops as a significant and chronic inflammatory response to inhaled irritants which ultimately leads to bronchial and alveolar remodelling in the lung[41] known as small airways disease.[132][133][134] Small airway disease (sometimes called chronic bronchiolitis) appears to be the precursor for the development of emphysema.[135] Airway remodelling with narrowing of peripheral airway and emphysema are responsible for the alteration of lung function in COPD.[136] Clearance of mucus from the airways is also altered with a dysregulation of cilia and mucus production.[137]
The inflammatory cells involved can include neutrophils, eosinophils, and macrophages, types of white blood cells. Those who smoke additionally have cytotoxic T cell involvement. Part of this cell response is brought on by inflammatory mediators such as chemotactic factors. Other processes involved with lung damage include oxidative stress produced by high concentrations of free radicals in tobacco smoke and released by inflammatory cells and breakdown of the connective tissue of the lungs by proteases (particularly elastase) that are insufficiently inhibited by protease inhibitors. The destruction of the connective tissue of the lungs leads to emphysema, which then contributes to the poor airflow and finally, poor absorption and release of respiratory gases. General muscle wasting that often occurs in COPD may be partly due to inflammatory mediators released by the lungs into the blood.[26]

Narrowing of the airways occurs due to inflammation and subsequent scarring within them. This contributes to the inability to breathe out fully. The greatest reduction in air flow occurs when breathing out, as the pressure in the chest is compressing the airways at this time. This can result in more air from the previous breath remaining within the lungs when the next breath is started, resulting in an increase in the total volume of air in the lungs at any given time, a process called air trapping which is closely followed by hyperinflation. Hyperinflation from exercise is linked to shortness of breath in COPD, as breathing in is less comfortable when the lungs are already partly filled. Hyperinflation may also worsen during an exacerbation.[138] There may also be airway hyperresponsiveness to irritants similar to those found in asthma.[119]
Low oxygen levels and eventually, high carbon dioxide levels in the blood, can occur from poor gas exchange due to decreased ventilation from airway obstruction, hyperinflation and a reduced desire to breathe.[26] During exacerbations, airway inflammation is also increased, resulting in increased hyperinflation, reduced expiratory airflow and worsening of gas transfer. This can lead to low blood oxygen levels, which, if present for a prolonged period, can result in narrowing of the arteries in the lungs, while emphysema leads to the breakdown of capillaries in the lungs. Both of these conditions may result in pulmonary heart disease also classically known as cor pulmonale.[47]
Diagnosis

The diagnosis of COPD should be considered in anyone over the age of 35 to 40 with shortness of breath, a chronic cough, coughing up of mucus, or frequent winter colds and a history of exposure to risk factors for the disease. Spirometry is then used to confirm the diagnosis.[4][139][140][4]
GOLD initially classified COPD in terms of a 4-level staging system based on severity of functional impairment.[11] The 2023 GOLD report introduced a new definition of COPD, a new taxonomic classification of COPD based on contributory causes or etiotypes, and revised recommendations for diagnosis and assessment.[12][15][18]
Spirometry
Spirometry measures the amount of airflow obstruction present and is generally carried out after the use of a bronchodilator, a medication to open up the airways.[141] Two main components are measured to make the diagnosis, the forced expiratory volume in one second (FEV1), which is the greatest volume of air that can be breathed out in the first second of a breath and the forced vital capacity (FVC), which is the greatest volume of air that can be breathed out in a single large breath.[142] Normally, 75–80% of the FVC comes out in the first second[142] and a FEV1/FVC ratio less than 70% in someone with symptoms of COPD defines a person as having the disease.[141][15] Because pulmonary function declines with ageing, use of this fixed threshold will lead to over-diagnosis of COPD in the elderly.[143][15] FEV1 is typically expressed as a percentage of the predicted "normal" for the person's age, gender, height and weight.[4] Airflow obstruction that is not fully reversible also can be found in patients with asthma and other diseases.[15] Testing the peak expiratory flow (the maximum speed of expiration), commonly used in asthma diagnosis, is not sufficient for the diagnosis of COPD.[144]
Internationally, definitions for diagnosis of COPD have changed over time.[145][146] The British Thoracic Society (BTS) has required both FEV1/ FVC <0.70 and an additional criterion of FEV1 <80% predicted, based on the Health Survey for England (HSfE).[145] National Institute for Health and Care Excellence (NICE) guidelines for COPD followed the BTS criteria as of 2010.[147] However, NICE was updated in 2019. NICE and GOLD are now in agreement in requiring only the presence of clinical symptoms confirmed by airflow obstruction with a reduced FEV1/FVC ratio less than 0.7.[145]
GOLD recommends further testing if symptoms seem out of proportion to degree of obstruction. Pulmonary function tests (PFTs) such as diffusing capacity of the lung for carbon monoxide, airway resistance, and respiratory oscillometry may help to better assess lung function by detecting static lung hyperinflation, airway obstruction, and small airway dysfunction.[143][146]
In those without symptoms, screening using spirometry is generally not recommended. However, active case finding and use of primary care data to identify those with risk factors, followed by spirometry, is recommended by GOLD 2024 as likely to lead to earlier diagnosis of COPD.[144][15]
Assessment
| Grade | Activity affected |
|---|---|
| 1 | Only strenuous activity |
| 2 | Vigorous walking |
| 3 | With normal walking |
| 4 | After a few minutes of walking |
| 5 | With changing clothing |
| Severity | FEV1% predicted |
|---|---|
| Mild (GOLD 1) | ≥80 |
| Moderate (GOLD 2) | 50–79 |
| Severe (GOLD 3) | 30–49 |
| Very severe (GOLD 4) | <30 |
A number of methods can be used to assess the effects and severity of COPD.[139][43] Use of screening questionnaires, such as the COPD diagnostic questionnaire (CDQ), alone or in combination with hand-held flow meters, is appropriate for screening of COPD in primary care.[148] The MRC breathlessness scale or the COPD assessment test (CAT) are simple questionnaires that may be used.[149][139] The St George Respiratory Questionnaire (SGRQ), can be used with patients who have chronic bronchitis to identify patients at risk of COPD exacerbation.[27]
Spirometry may help to determine the severity of airflow limitation.[4] GOLD also refers to a modified MRC scale that is simply a test of breathlessness experienced.[43][150] Scores on CAT range from 0–40 with the higher the score, the more severe the disease.[151]
As of 2023, GOLD updated its guidelines, revising its assessment approach. Once a COPD diagnosis has been confirmed by spirometry, assessment focuses on the degree of airflow limitation, type and degree of other current symptoms, history of exacerbations, and multimorbidities. GOLD's 2023 model recognizes that exacerbations are an important risk factor independent of the level of other symptoms. Patients are classed as A, B, or E. Patients are considered class E if they have a history in the past year of 1 or more exacerbations leading to hospitalization, or 2 or more moderate exacerbations. Patients in Class A or B cannot have more than 1 moderate or severe exacerbation in the past year, not requiring hospital admission. Patients in Class A display a low symptom burden and low exacerbation risk Patients in Class B display a higher symptom burden. Initial pharmacological treatment guidelines are suggested based on presence in these categories.[15][152]
Other tests
A chest X-ray is not useful to establish a diagnosis of COPD, but it can be used in either excluding other conditions or including comorbidities such as pulmonary fibrosis and bronchiectasis. Characteristic signs of COPD on X-ray include hyperinflation (shown by a flattened diaphragm and an increased retrosternal air space) and lung hyperlucency.[5] A saber-sheath trachea is a tracheal deformity that is also indicative of COPD.[153]
A CT scan is not routinely used except for the exclusion of bronchiectasis.[5] Pulse oximetry measurement of peripheral oxygen saturation is recommended in people with clinical signs of respiratory failure or right heart failure.[5] An analysis of arterial blood is recommended in those with a peripheral oxygen saturation of 92% or less to determine actual blood oxygen level and assess for high levels of carbon dioxide in the blood, which may have therapeutic implications such as need for non-invasive ventilation or oxygen supplementation.[19] WHO recommends that all those diagnosed with COPD be screened for alpha-1 antitrypsin deficiency.[43]
-
 Chest X-ray demonstrating severe COPD, displaying small heart size in comparison to the lungs
Chest X-ray demonstrating severe COPD, displaying small heart size in comparison to the lungs -
 A lateral chest X-ray of a person with emphysema, displaying barrel chest and flat diaphragm
A lateral chest X-ray of a person with emphysema, displaying barrel chest and flat diaphragm -
 Lung bulla as seen on chest X-ray in a person with severe COPD
Lung bulla as seen on chest X-ray in a person with severe COPD -
 A severe case of bullous emphysema
A severe case of bullous emphysema -
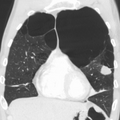
 Axial CT image of the lung of a person with end-stage bullous emphysema
Axial CT image of the lung of a person with end-stage bullous emphysema -
 Very severe emphysema with lung cancer on the left (CT scan)
Very severe emphysema with lung cancer on the left (CT scan)






Differential diagnosis
COPD may need to be differentiated from other conditions such as congestive heart failure, asthma, bronchiectasis, tuberculosis, obliterative bronchiolitis, lung cancer, and diffuse panbronchiolitis.[5] The key distinction between asthma and COPD is that in asthma lung function should show significant improvement or return to normal with regular inhaled corticosteroid treatment.[144] Airflow limitation that disappears following use of bronchodilators is incompatible with a diagnosis of COPD.[15] Chronic bronchitis with normal airflow (NOCB) is not classified as COPD. However, those with NOCB have an increased risk of developing COPD and higher mortality.[154]
Prevention
Many cases of COPD are potentially preventable through decreasing exposure to tobacco smoke and other indoor and outdoor pollutants.[155] It also may be possible to prevent development of COPD in later life by improving conditions that affect lung development in early life, such as frequent respiratory illness, poor nutrition, low physical activity, and early alcohol consumption.[17]
Smoking cessation
The policies of governments, public health agencies and antismoking organizations can reduce smoking rates by discouraging people from starting and encouraging people to stop smoking.[156] Smoking bans in public areas and places of work are important measures to decrease exposure to secondhand smoke, and while many places have instituted bans, more are recommended.[104]
In those who smoke, stopping smoking is a crucial strategy shown to slow down the worsening of COPD.[157][158][159] In the short term, quitting smoking can reduce respiratory symptoms. In the longer term, quitting can improve lung function, exercise capacity, perceived quality of life, and survival of those with COPD.[157] It can reduce flare-ups and hospitalizations.[160] Even at a late stage of the disease, it can reduce the rate of worsening lung function and delay the onset of disability and death.[157] Quitting earlier in life and not smoking for longer periods (>10 years) show greater benefits.[160]
Often, several attempts are required before long-term abstinence is achieved.[156] Attempts over 5 years lead to success in nearly 40% of people.[161][157] Some smokers can achieve long-term smoking cessation through willpower alone. Smoking, however, is highly addictive, and many smokers need further support.[162] The chance of quitting is improved with social support, engagement in a smoking cessation program and the use of medications such as nicotine replacement therapy, bupropion, or varenicline.[156][159][161] Combining smoking-cessation medication with behavioral therapy is more than twice as likely to be effective in helping people with COPD stop smoking, compared with behavioral therapy alone.[163]
Occupational health
Measures to reduce occupation exposure in at-risk industries include public policy and regulation to support healthy workplaces; identifying risky work settings and exposures; actionable steps to reduce exposure to risk factors and triggers for flare-ups; education of workers, management and medical professionals about risks, diagnosis, and management; promoting smoking cessation; checking workers for early signs of COPD; and using equipment such as respirators for better control of dust and gases.[164][13][165][166][167] Employers must provide a safe working environment, safeguarding employees through the use of ventilation, personal protection equipment, and regular air quality monitoring.[165] Improving ventilation and using water spraying and dust suppressant techniques can help to reduce respirable dust. Education and training are important in ensuring that methods are properly used.[168]
Pollution control
Both indoor and outdoor air quality can be improved, which may prevent COPD and slow the worsening of existing disease. This may be achieved through public policy efforts, cultural changes and personal involvement.[155][169][170] Some countries have successfully improved outdoor air quality through regulations, resulting in improvements in the lung function of their populations.[95]
Cities or other organizations may monitor air quality, sometimes sharing data with the public through air quality indices and alerts.[171][172] Individuals are often advised to avoid or reduce exposure to irritants in indoor and outdoor pollution through smoking cessation, engaging in activities at times and places when exposure to pollutants is lower, and using protective gear (e.g. N95 masks, air filtration).[155] It is becoming increasingly possible to monitor individual exposures to air pollution and adapt behavior accordingly.[173][174]
In developing countries, a key effort is to reduce exposure to smoke from cooking and heating fuels through improved ventilation of homes and user of cleaner fuels, stoves and chimneys.[155][175] Proper stoves may improve indoor air quality by 85%. Using alternative energy sources such as solar cooking and electrical heating is also effective.[104] However, poverty is often a barrier to the adoption of better fuels. Higher-income families may use modern fuels such as natural gas or electricity, which cause less pollution and can lead to better health outcomes. Electricity supply, however, is often insufficient to meet a family's heating needs. If electricity is supplemented with low-quality biofuels, indoor air-pollution levels will increase and negatively affect health outcomes.[175]
Management
COPD currently has no cure,[176] but the symptoms are treatable and its progression can be delayed, particularly by stopping smoking.[1][6] If COPD is detected early, while symptoms are still mild, interventions to prevent decline in lung function have a greater effect. For both individual treatment and public health, early diagnosis and intervention are recommended.[7][13][177] Emphasis has shifted to early prevention, treatment, and disease stabilization, with goals of improving quality of life and reducing flare-ups (exacerbations).[14] In cases of early and mild COPD, pulmonary rehabilitation may help to improve exercise capacity and quality of life.[7][13][177]
A major goal of management is to reduce exposure to risk factors including offering non-pharmacological treatments such as help with stopping smoking. Stopping smoking can reduce the rate of lung function decline and also reduce mortality from smoking-related diseases such as lung cancer and cardiovascular disease.[1] Other recommendations include pneumococcal vaccination and yearly influenza vaccination to help reduce the risk of flare-ups; as of 2024 CDC and GOLD also recommend RSV vaccine for individuals above 60 years.[178][19] Guidance is also advised as to managing breathlessness and stress.[6]
Multiple illnesses often need to be managed along with COPD. An important approach is the use of an action plan. which is drawn up and reviewed with the patient and caregivers.[155] Providing people with a personalized action plan, education and support for use of their action plan in the event of an flare-up, can reduce hospital visits and encourage early treatment of such exacerbations.[179][180] When self-management interventions, such as taking corticosteroids and using supplemental oxygen, are combined with action plans, health-related quality of life is improved compared to usual care.[181] In those with COPD who are malnourished, supplementation with vitamin C, vitamin E, zinc and selenium can improve weight, strength of respiratory muscles and health-related quality of life.[182] Significant vitamin D deficiency is common in those with COPD and can cause increased exacerbations. Supplementation when deficient can give a 50% reduction in the number of exacerbations.[29][183]
Several medical treatments are used in the management of stable COPD and exacerbations. These include bronchodilators, corticosteroids and antibiotics.
In hospitalized patients and those with a severe exacerbation, antibiotics can improve outcomes.[184][185] The macrolide class of antibiotics (e.g. azithromycin) has been shown to be effective in reducing frequency of exacerbations.[98][186] There is no clear evidence of improved outcomes for their use with less severe cases.[184] Routine use of antibiotics is not recommended in mild or outpatient cases without signs of bacterial infection.[185] The FDA recommends against the use of fluoroquinolones when other options are available due to higher risks of serious side effects.[187]
Non-invasive ventilation may be used to support breathing and also reduce daytime breathlessness.[188][182] Patients with COPD exacerbations can display acute hypercapnic respiratory failure (acutely raised levels of carbon dioxide). Bilevel positive airway pressure (BPAP) is preferred to continuous positive airway pressure (CPAP) in treating cases of cardiogenic pulmonary edema with hypercapnia.[189][190]
In those with end-stage disease, palliative care is focused on relieving symptoms.[191] Morphine can improve exercise tolerance.[182]
Bronchodilators
Inhaled short-acting bronchodilators are the primary medications used on an as needed basis; their use regularly is not recommended.[6] The two major types are beta2-adrenergic agonists and anticholinergics; either in long-acting or short-acting forms.[14]
COPD is heterogeneous, and treatment must be individualized.[14] Beta2–adrenergic agonists target receptors in the smooth muscle cells in bronchioles causing them to relax and allow improved airflow. They reduce shortness of breath, tend to reduce dynamic hyperinflation and improve exercise tolerance.[6][192] Short-acting bronchodilators have an effect for four hours and for maintenance therapy long acting bronchodilators with an effect of over twelve hours are used. In times of more severe symptoms, a short-acting agent may be used in combination.[6] An inhaled corticosteroid used with a long-acting beta-2 agonist is more effective than either one on its own.[193] The 2018 NICE guideline recommends use of dual long-acting bronchodilators with economic modelling suggesting that this approach is preferable to starting one long-acting bronchodilator and adding another later.[194]
The GOLD 2022 report recommends pharmacological treatment with a long-acting muscarinic antagonist (LAMA) such as tiotropium or a long-acting beta agonist (LABA) as initial monotherapy for most patients. Dual bronchodilator therapy (LABA+LAMA) is recommended for more severe symptoms.[195] Other guidelines vary in recommending whether to try LABA or LAMA first.[195] The GOLD 2023 report suggests trying either LAMA or LABA for patients in Class A; using combined LAMA+LABA for those in Group B or E; and LAMA+LABA+ICS for those in Group E with high blood eosinophil counts.[15] American Thoracic Society guidelines strongly recommend LABA+LAMA combination therapy over LAMA or LABA monotherapy in patients with COPD and dyspnea or exercise intolerance.[195] The combination of LABA+LAMA may reduce COPD exacerbations and improve quality-of-life compared to long-acting bronchodilators alone.[196]
Several short-acting β2 agonists are available, including salbutamol (albuterol) and terbutaline.[6] They provide relief of symptoms for four to six hours.[6] A long-acting beta agonist (LABA) such as salmeterol, formoterol and indacaterol is often used as maintenance therapy, with a duration of action of 12 to 24 hours.[6] Indacaterol requires an inhaled dose once a day and is as effective as the other long-acting β2 agonist drugs that require twice-daily dosing for people with stable COPD.[197] Long-term use of LABAs and LAMAs separately or in combination appear safe for COPD, with combination therapy improving lung function and quality of life and reducing COPD symptoms, first moderate/severe exacerbation risk, risk of first clinically important deterioration (CID), and use of rescue medication.[198][199][200] In severe cases, triple therapy of LABA+LAMA with inhaled steroids (ICS) has some evidence of benefits.[201] In patients with a high risk of pneumonia, LABA+LAMA may be a safer treatment option than all three together (LABA+LAMA+ICS) since adding ICS increases the risk of pneumonia.[199][200]
The two main anticholinergics used in COPD are ipratropium and tiotropium. Ipratropium is a short-acting muscarinic antagonist (SAMA), while tiotropium is long-acting muscarinic antagonist (LAMA). Tiotropium is associated with improved lung function, quality of life, and exercise endurance, and reduced shortness of breath, hyperinflation, exacerbations, rescue medication use, hospitalization rates, and mortality. Tiotropium provides those benefits better than ipratropium.[202] Anticholinergics can cause dry mouth,[202] and urinary tract symptoms (in men) .[203] Long-acting antimuscarinic agents (LAMA) have not been found to be associated with increased risk of heart disease.[204] Aclidinium, another long-acting agent, also shows less shortness of breath, increases in lung function and improved quality of life.[205] The LAMA umeclidinium bromide is another anticholinergic alternative.[206] When compared to tiotropium, the LAMAs aclidinium, glycopyrronium, and umeclidinium appear to have a similar level of efficacy, with all four being more effective than placebo.[207]
Corticosteroids
Inhaled corticosteroids are anti-inflammatories that are recommended by GOLD as a first-line maintenance treatment in COPD cases with repeated flare-ups.[208][209] Their regular use increases the risk of pneumonia in severe cases.[29] Studies have shown that the risk of pneumonia is associated with all types of corticosteroids: it is related to the disease severity and a dose-response relationship has been noted.[208] Oral glucocorticoids can be effective in treating an acute exacerbation.[193] They appear to have fewer side effects than those given intravenously.[210] Five days of steroids work as well as ten or fourteen days.[211]
The use of corticosteroids is associated with a decrease in the number of lymphoid follicles (in the bronchial lymphoid tissue).[135] A triple inhaled therapy of LABA/LAMA/ICS improves lung function, reduces symptoms and exacerbations and is seen to be more effective than mono or dual therapies.[212][193] NICE guidelines recommend the use of ICSs in people with asthmatic features or features suggesting steroid responsiveness.[194]
PDE4 inhibitors
Phosphodiesterase-4 inhibitors (PDE4 inhibitors) are anti-inflammatories that improve lung function and reduce exacerbations in moderate to severe illness. Roflumilast is a PDE4 inhibitor used orally once daily to reduce inflammation; it has no direct bronchodilatory effects. It is essentially used in treating those with chronic bronchitis along with systemic corticosteroids.[213] Reported adverse effects of roflumilast appear early in treatment, become less with continued treatment and are reversible. One effect is dramatic weight loss, and its use is to be avoided in underweight people. It is also advised to be used with caution in those who have depression.[213]
Other medications
Long-term preventive use of antibiotics, is not recommended in COPD patients with frequent exacerbations.[18][214] A major concern is the development of bacterial resistance, which has been shown. Long-term use may also reduce microbial diversity in the respiratory tract. Other side effects include hearing loss,[214] tinnitus and changes to the heart rhythm known as long QT syndrome.[215]
There is evidence that the macrolide class of antibiotics (e.g. azithromycin, clarithromycin, erythromycin) is effective in reducing frequency of exacerbations.[214][186][215] Whether this is a result of antibacterial or immunomodulant properties is not clear. Effects on airway inflammation are uncertain, but reductions in neutrophil cell counts are significant.[214] Azithromycin has been suggested as the most promising of the macrolides due to better patient adherence, dose management, and tolerability of side effects. However, administration should be very cautious: serious side effects can occur, including increases in antibiotic resistance.[214] Roxithromycin, a macrolide, and moxifloxacin, a quinolone, did not significantly improve exacerbation rates.[214][186] Moxifloxacin and doxycycline may even increase exacerbation rates, suggesting these classes (fluoroquinolones and tetracyclines) are ineffective.[214][186]
Methylxanthines such as theophylline are widely used. Theophylline is seen to have a mild bronchodilatory effect in stable COPD. Inspiratory muscle function is seen to be improved, but the causal effect is unclear. Theophylline is seen to improve breathlessness when used as an add-on to salmeterol. All instances of improvement have been reported using sustained-release preparations.[6] Methylxanthines are not recommended for use in exacerbations due to adverse effects.[29]
Mucolytics may help to reduce exacerbations in some people with chronic bronchitis, as noticed by fewer hospitalizations and fewer days of disability in one month.[216] Erdosteine is recommended by NICE.[217] GOLD also supports the use of some mucolytics that are advised against when inhaled corticosteroids are being used and singles out erdosteine as having good effects regardless of corticosteroid use. Erdosteine also has antioxidant properties, but there is not enough evidence to support the general use of antioxidants.[213] Erdosteine has been shown to significantly reduce the risk of exacerbations, shorten their duration and hospital stays.[218]
Cough medicines are not recommended.[219] Beta blockers are not contraindicated for those with COPD and should only be used where there is concomitant cardiovascular disease.[213]
Recent studies show that metformin plays a role in reducing systemic inflammation by reducing biomarker levels that are increased during COPD exacerbations.[220]
Oxygen therapy
Supplemental oxygen is recommended for those with low oxygen levels in respiratory failure at rest (a partial pressure of oxygen less than 50–55 mmHg or oxygen saturations of less than 88%).[182] When taking into account complications including cor pulmonale and pulmonary hypertension, the levels involved are 56–59 mmHg.[221] Oxygen therapy is to be used for between 15 and 18 hours per day and is said to decrease the risk of heart failure and death.[221] In those with normal or mildly low oxygen levels, oxygen supplementation (ambulatory) may improve shortness of breath when given during exercise, but may not improve breathlessness during normal daily activities or affect the quality of life.[222] During acute exacerbations, many require oxygen therapy; the use of high concentrations of oxygen without taking into account a person's oxygen saturations may lead to increased levels of carbon dioxide and worsened outcomes.[223][224] In those at high risk of high carbon dioxide levels, oxygen saturations of 88–92% are recommended, while for those without this risk, recommended levels are 94–98%.[224] Once prescribed long-term oxygen therapy, patients should be re-assessed after 60 to 90 days, to determine whether supplemental oxygen is still indicated and if prescribed supplemental oxygen is effective.[19][225]
Rehabilitation
Pulmonary rehabilitation is a program of exercise, disease management and counseling, coordinated to benefit the individual.[226] A severe exacerbation leads to hospital admission, high mortality and a decline in the ability to carry out daily activities. Following a hospital admission, pulmonary rehabilitation has been shown to significantly reduce future hospital admissions, mortality and improve quality of life.[63]
The optimal exercise routine, use of noninvasive ventilation during exercise and intensity of exercise suggested for people with COPD, is unknown.[227][228] Performing endurance arm exercises improves arm movement for people with COPD and may result in a small improvement in breathlessness.[229] Performing arm exercises alone does not appear to improve quality of life.[229] Pursed-lip breathing exercises may be useful.[22] Tai chi exercises appear to be safe to practice for people with COPD and may be beneficial for pulmonary function and pulmonary capacity when compared to a regular treatment program.[230] Tai Chi was not found to be more effective than other exercise intervention programs.[230] Inspiratory and expiratory muscle training (IMT, EMT) have been suggested and may provide some improvements when compared to no treatment.[231] A combination of IMT and walking exercises at home may help limit breathlessness in cases of severe COPD.[232] Additionally, the use of low amplitude high velocity joint mobilization together with exercise improves lung function and exercise capacity.[233] The goal of spinal manipulation therapy is to improve thoracic mobility in an effort to reduce the work on the lungs during respiration, however, the evidence supporting manual therapy for people with COPD is very weak.[233][234]
Airway clearance techniques (ACTs), such as postural drainage, percussion/vibration, autogenic drainage, hand-held positive expiratory pressure (PEP) devices and other mechanical devices, may reduce the need for increased ventilatory assistance, the duration of ventilatory assistance and the length of hospital stay in people with acute COPD.[235] In people with stable COPD, ACTs may lead to short-term improvements in health-related quality of life and a reduced long-term need for hospitalizations related to respiratory issues.[235]
Being either underweight or overweight can affect the symptoms, degree of disability and prognosis of COPD. People with COPD who are underweight can improve their breathing muscle strength by increasing their calorie intake. When combined with regular exercise or a pulmonary rehabilitation program, this can lead to improvements in COPD symptoms. Supplemental nutrition may be useful in those who are malnourished.[182][236]
Management of exacerbations
People with COPD can experience exacerbations (flare-ups) that commonly start with respiratory tract infections. The symptoms that worsen are not specific to COPD and differential diagnoses need to be considered.[29] Acute exacerbations are typically treated by increasing the use of short-acting bronchodilators, including a combination of a short-acting inhaled beta agonist and short-acting anticholinergic.[29] These medications can be given either via a metered-dose inhaler with a spacer or via a nebulizer, with both appearing to be equally effective.[213][237] Nebulization may be easier for those who are more unwell.[213] Oxygen supplementation can be useful. Excessive oxygen; however, can result in increased CO
2 levels and a decreased level of consciousness.[238] Corticosteroids given orally can improve lung function and shorten hospital stays but their use is recommended for only five to seven days; longer courses increase the risk of pneumonia and death.[29]
Room temperature
Maintaining room temperature of at least 21 °C (70 °F) for a minimum of nine hours a day was associated with better health in those with COPD, especially for smokers.[239] The World Health Organization (WHO) recommends indoor temperatures of a slightly higher range between 18 and 24 °C (64 and 75 °F).[240]
Room humidity
For people with COPD, the ideal indoor humidity levels are 30–50% RH. Maintaining indoor humidity can be difficult in the winter, especially in cold climates where the heating system is constantly running.[241]
Keeping the indoor relative humidity above 40% RH significantly reduces the infectivity of aerosolized viruses.[242]
Procedures for emphysema
There are several procedures to reduce the volume of a lung in cases of severe emphysema with hyperinflation.
Surgical
For severe emphysema that has proved unresponsive to other therapies lung volume reduction surgery (LVRS) may be an option.[243][244] LVRS involves the removal of damaged tissue, which improves lung function by allowing the rest of the lungs to expand.[190] It is considered when the emphysema is in the upper lobes and when there are no comorbidities.[245]
Bronchoscopic
Minimally invasive bronchoscopic procedures may be carried out to reduce lung volume. These include the use of valves, coils, or thermal ablation.[182][246] Endobronchial valves are one-way valves that may be used in those with severe hyperinflation resulting from advanced emphysema; a suitable target lobe and no collateral ventilation are required for this procedure. The placement of one or more valves in the lobe induces a partial collapse of the lobe that ensures a reduction in residual volume that improves lung function, the capacity for exercise and quality of life.[247]
The placement of nitinol coils instead of valves is recommended where there is collateral ventilation that would prevent the use of valves.[248] Nitinol is a biocompatible alloy.
Both of these techniques are associated with adverse effects, including persistent air leaks and cardiovascular complications. Thermal vapor ablation has an improved profile. Heated water vapor is used to target lobe regions, which leads to permanent fibrosis and volume reduction. The procedure can target individual lobe segments, can be carried out regardless of collateral ventilation, and can be repeated with the natural advance of emphysema.[249]
Other surgeries
In very severe cases, lung transplantation might be considered.[243] A CT scan may be useful in surgery considerations.[113] Ventilation/perfusion scintigraphy is another imaging method that may be used to evaluate cases for surgical interventions and also to evaluate post-surgery responses.[250] A bullectomy may be carried out when a giant bulla occupies more than a third of a hemithorax.[245]
Prognosis


| no data ≤110 110–220 220–330 330–440 440–550 550–660 | 660–770 770–880 880–990 990–1100 1100–1350 ≥1350 |
COPD is progressive and can lead to premature death. It is estimated that 3% of all disability is related to COPD.[252] The proportion of disability from COPD globally has decreased from 1990 to 2010 due to improved indoor air quality primarily in Asia.[252] The overall number of years lived with disability from COPD, however, has increased.[253]
There are many variables affecting the long-term outcome in COPD and GOLD recommends the use of a composite test (BODE) that includes the main variables of body-mass index, obstruction of airways, dyspnea (breathlessness) and exercise and not just spirometry results.[43] NICE recommends against the use of BODE for the prognosis assessment in stable COPD; factors such as exacerbations and frailty need to be considered.[246] Other factors that contribute to a poor outcome include older age, comorbidities such as lung cancer and cardiovascular disease and the number and severity of exacerbations needing hospital admission.[29]
Epidemiology
Estimates of prevalence have considerable variation due to differences in analytical and surveying approach and the choice of diagnostic criteria.[254] An estimated 213 million people had COPD in 2021, corresponding to a global prevalence of 2.7%,[9] whereas epidemiological studies indicated an estimation of 384 million having COPD in 2010, corresponding to a global prevalence of 12%.[11]
The disease affects both men and women[3] but risk is heavily influenced by age, gender, lifestyle, and socioeconomic factors,[8][125][255] and prevalence varies with countries and regions.[255] A higher rate of COPD is found in those over 40 years and this increases greatly with advancing age with the highest rate found in those over 60 years.[11] When exposure factors are equal, women tend to be at higher risk of COPD, possibly reflecting sex differences in the anatomy of the respiratory system.[131] In never-smokers, COPD is more common in women than men.[8] However, men are more likely to smoke, the top risk factor.[8]
A review of data from 201 countries between 1990 to 2021 shows a variety of changes in age-standardized prevalence and death rates of COPD. Rates in some countries increased, some were stable, and some decreased. Changes in prevalence appear to reflect changes in rates of smoking and air polliution. In addition, the use of biomass fuels for cooking is related to increased COPD prevalence, particularly in women, while gas cooking is related to reduced prevalence. The universal thermal climate index and various climatic conditions also correlate with COPD prevalence.[255] Globally, incidence and mortality rates declined slightly between 1990 and 2021, but this was not true for all demographics.[255][256]
In 2023, COPD was the third-leading cause of death globally.[257] In low-income countries, COPD does not appear in the Top 10 causes of death; in other income groups, it is in the Top 5.[258] Around three million people die of COPD each year.[11] Tobacco use, ambient air pollution, and socioeconomic factors are all associated with higher death rates.[255] In some countries, mortality has decreased in men but increased in women.[259][257] This may reflect rates of smoking in women and men becoming more similar.[259]
In the UK, three million people are reported to be affected by COPD – two million of these being undiagnosed. On average, the number of COPD-related deaths between 2007 and 2016 was 28,600. The estimated number of deaths due to occupational exposure was estimated to be about 15% at around 4,000.[254]
In the United States in 2018, almost 15.7 million people had been diagnosed with COPD and it is estimated that millions more have not been diagnosed.[260] In the United States in 2021, about 11.7 million insured individuals were identified with COPD. There were 1.8 million COPD-related acute inpatient hospitalizations. Both COPD prevalence and COPD-related hospitalization rates varied widely among states.[261]
History

The name chronic obstructive pulmonary disease is believed to have first been used in 1965.[262] Previously it has been known by a number of different names, including chronic obstructive bronchopulmonary disease, chronic airflow obstruction, chronic obstructive lung disease, nonspecific chronic pulmonary disease, and diffuse obstructive pulmonary syndrome.[262]
The terms emphysema and chronic bronchitis were formally defined as components of COPD in 1959 at the CIBA guest symposium and in 1962 at the American Thoracic Society Committee meeting on Diagnostic Standards.[262]
Early descriptions of probable emphysema began in 1679 by T. Bonet of a condition of "voluminous lungs" and in 1769 by Giovanni Morgagni of lungs which were "turgid particularly from air".[262][263] In 1721, the first drawings of emphysema were made by Ruysh.[263] René Laennec, used the term emphysema in his book A Treatise on the Diseases of the Chest and of Mediate Auscultation (1837) to describe lungs that did not collapse when he opened the chest during an autopsy. He noted that they did not collapse as usual because they were full of air and the airways were filled with mucus.[262] In 1842, John Hutchinson invented the spirometer, which allowed the measurement of vital capacity of the lungs. However, his spirometer could only measure volume, not airflow. Tiffeneau and Pinelli in 1947 described the principles of measuring airflow.[262]
Air pollution and the increase in cigarette smoking in Great Britain at the start of the 20th century led to high rates of chronic lung disease, though it received little attention until the Great Smog of London in December 1952. This spurred epidemiological research in the United Kingdom, Holland and elsewhere.[264] In 1953, George L. Waldbott, an American allergist, first described a new disease he named smoker's respiratory syndrome in the 1953 Journal of the American Medical Association. This was the first association between tobacco smoking and chronic respiratory disease.[265]
Modern treatments were developed during the second half of the 20th century. Evidence supporting the use of steroids in COPD was published in the late 1950s. Bronchodilators came into use in the 1960s following a promising trial of isoprenaline. Further bronchodilators, such as short-acting salbutamol, were developed in the 1970s and the use of long-acting bronchodilators began in the mid-1990s.[266]
Society and culture
It is generally accepted that COPD is widely underdiagnosed and many people remain untreated. In the US the NIH has promoted November as COPD Awareness Month to be an annual focus on increasing awareness of the condition.[267]
Economics
Globally, as of 2010, COPD is estimated to result in economic costs of $2.1 trillion, half of which occurring in the developing world.[268] Of this total an estimated $1.9 trillion are direct costs such as medical care, while $0.2 trillion are indirect costs such as missed work.[269] This is expected to more than double by 2030.[268] In Europe, COPD represents 3% of healthcare spending.[11] In the United States, costs of the disease were estimated at $50 billion in 2010, most of which is due to exacerbation.[11] In the United Kingdom this cost was in 2021 estimated at £3.8 billion annually.[270]
Research
Stem-cell therapy using mesenchymal stem cells was in June 2021 studied in eight clinical trials had been completed and seventeen were underway.[271]
The effectiveness of alpha-1 antitrypsin augmentation treatment for people who have alpha-1 antitrypsin deficiency is unclear.[272][12][52][19][70]
Metabolomic approaches to diagnosing and differentiating subtypes of COPD are being studied.[273][274][275]
Research continues into the use of telehealthcare to treat people with COPD when they experience episodes of shortness of breath; treating people remotely may reduce the number of emergency-room visits and improve the person's quality of life.[276]
American people with COPD and their caregivers consider the following COPD-related research areas as the most important: family/social/community research, well-being of people with COPD, curative research, biomedical therapies, policy, and holistic therapies.[277]
Other animals
Chronic obstructive pulmonary disease may occur in a number of other animals and may be caused by exposure to tobacco smoke.[278] In horses it is known as recurrent airway obstruction (RAO) or heaves. RAO can be quite severe and most often is linked to exposure to common allergens.[279] COPD is also commonly found in old dogs.[280]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 "Chronic obstructive pulmonary disease". https://cks.nice.org.uk/topics/chronic-obstructive-pulmonary-disease/.
- ↑ 2.0 2.1 2.2 "Chronic obstructive pulmonary disease (COPD) — Complications". BMJ Best Practice. https://bestpractice.bmj.com/topics/en-gb/7/complications.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 "Chronic obstructive pulmonary disease (COPD)" (in en). Fact Sheets. World Health Organization. 2024-11-06. https://www.who.int/en/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
- ↑ 4.00 4.01 4.02 4.03 4.04 4.05 4.06 4.07 4.08 4.09 4.10 Gold Report 2021, pp. 20–27, Chapter 2: Diagnosis and initial assessment.
- ↑ 5.0 5.1 5.2 5.3 5.4 Gold Report 2021, pp. 33–35, Chapter 2: Diagnosis and initial assessment.
- ↑ 6.00 6.01 6.02 6.03 6.04 6.05 6.06 6.07 6.08 6.09 6.10 6.11 Gold Report 2021, pp. 40–46, Chapter 3: Evidence supporting prevention and maintenance therapy.
- ↑ 7.00 7.01 7.02 7.03 7.04 7.05 7.06 7.07 7.08 7.09 7.10 Murgia, N; Gambelunghe, A; Stirnemann, H (June 2022). "Occupational COPD-The most under-recognized occupational lung disease?". Respirology 27 (6): 399–410. doi:10.1111/resp.14272. PMID 35513770.
- ↑ 8.0 8.1 8.2 8.3 8.4 8.5 8.6 8.7 8.8 Mălăescu, AN; Mihălțan, FD; Constantin, AA (26 December 2025). "Chronic Obstructive Pulmonary Disease in Never-Smokers-A Distinct Entity Within the COPD Spectrum.". Life 16 (1): 43. doi:10.3390/life16010043. PMID 41598199. Bibcode: 2025Life...16...43M.
- ↑ 9.0 9.1 9.2 9.3 ((GBD 2021 Diseases and Injuries Collaborators)) (2024-05-18). "Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021". The Lancet 403 (10440): 2133–2161. doi:10.1016/S0140-6736(24)00757-8. ISSN 0140-6736. PMID 38582094.
- ↑ ((GBD 2021 Causes of Death Collaborators)) (2024-05-18). "Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021". The Lancet 403 (10440): 2100–2132. doi:10.1016/S0140-6736(24)00367-2. ISSN 0140-6736. PMID 38642570. Bibcode: 2024Lanc..403.2100N.
- ↑ 11.00 11.01 11.02 11.03 11.04 11.05 11.06 11.07 11.08 11.09 11.10 11.11 11.12 11.13 11.14 Gold Report 2021, pp. 4–8, Chapter 1: Definition and overview.
- ↑ 12.00 12.01 12.02 12.03 12.04 12.05 12.06 12.07 12.08 12.09 12.10 12.11 12.12 12.13 12.14 12.15 12.16 12.17 Xie, C; Wang, K; Yang, K; Zhong, Y; Gul, A; Luo, W; Yalikun, M; He, J et al. (29 September 2025). "Toward precision medicine in COPD: phenotypes, endotypes, biomarkers, and treatable traits.". Respiratory Research 26 (1): 274. doi:10.1186/s12931-025-03356-w. PMID 41024111.
- ↑ 13.0 13.1 13.2 13.3 13.4 13.5 13.6 13.7 13.8 Vogelmeier, CF; Friedrich, FW; Timpel, P; Kossack, N; Diesing, J; Pignot, M; Abram, M; Gediga, M et al. (2025). "Comorbidities and Cause of Death in COPD Patients Compared to Non-COPD Controls: An 8-year Observational Retrospective Healthcare Claims Database Cohort Study.". International Journal of Chronic Obstructive Pulmonary Disease 20: 2117–2130. doi:10.2147/COPD.S488701. PMID 40606812.
- ↑ 14.0 14.1 14.2 14.3 Duan, R; Li, B; Yang, T (June 2023). "Pharmacological therapy for stable chronic obstructive pulmonary disease.". Chronic Diseases and Translational Medicine 9 (2): 82–89. doi:10.1002/cdt3.65. PMID 37305108.
- ↑ 15.0 15.1 15.2 15.3 15.4 15.5 15.6 15.7 15.8 Agustí, A; Celli, BR; Criner, GJ; Halpin, D; Anzueto, A; Barnes, P; Bourbeau, J; Han, MK et al. (1 April 2023). "Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary.". American Journal of Respiratory and Critical Care Medicine 207 (7): 819–837. doi:10.1164/rccm.202301-0106PP. PMID 36856433.
- ↑ 16.0 16.1 16.2 16.3 Cronin, E; Cushen, B (January 2025). "Diagnosis and management of comorbid disease in COPD.". Breathe (Sheffield, England) 21 (1): 240099. doi:10.1183/20734735.0099-2024. PMID 40007528.
- ↑ 17.0 17.1 17.2 17.3 17.4 17.5 17.6 17.7 17.8 Agustí, A; Melén, E; DeMeo, DL; Breyer-Kohansal, R; Faner, R (May 2022). "Pathogenesis of chronic obstructive pulmonary disease: understanding the contributions of gene-environment interactions across the lifespan.". The Lancet. Respiratory Medicine 10 (5): 512–524. doi:10.1016/S2213-2600(21)00555-5. PMID 35427533.
- ↑ 18.0 18.1 18.2 18.3 "2023 GOLD Report" (in en-US). 2024-11-15. https://goldcopd.org/2023-gold-report/.
- ↑ 19.0 19.1 19.2 19.3 19.4 19.5 "2025 GOLD Report" (in en-US). 2024-11-15. https://goldcopd.org/2025-gold-report/.
- ↑ Singh, D; Higham, A; Mathioudakis, AG; Beech, A (July 2025). "Chronic Obstructive Pulmonary Disease (COPD): Developments in Pharmacological Treatments.". Drugs 85 (7): 911–930. doi:10.1007/s40265-025-02188-8. PMID 40392521.
- ↑ Khan, KS; Jawaid, S; Memon, UA; Perera, T; Khan, U; Farwa, UE; Jindal, U; Afzal, MS et al. (August 2023). "Management of Chronic Obstructive Pulmonary Disease (COPD) Exacerbations in Hospitalized Patients From Admission to Discharge: A Comprehensive Review of Therapeutic Interventions.". Cureus 15 (8). doi:10.7759/cureus.43694. PMID 37724212.
- ↑ 22.0 22.1 "Effects of acute use of pursed-lips breathing during exercise in patients with COPD: a systematic review and meta-analysis". Physiotherapy 104 (1): 9–17. March 2018. doi:10.1016/j.physio.2017.08.007. PMID 28969859.
- ↑ Gold Report 2021, pp. 90–96, Chapter 4: Management of stable COPD.
- ↑ "Dyspnea in COPD: New Mechanistic Insights and Management Implications". Advances in Therapy 37 (1): 41–60. January 2020. doi:10.1007/s12325-019-01128-9. PMID 31673990.
- ↑ 25.0 25.1 "Chronic Obstructive Pulmonary Disease: Epidemiology, Biomarkers, and Paving the Way to Lung Cancer". J Clin Med 10 (13): 2889. June 2021. doi:10.3390/jcm10132889. PMID 34209651.
- ↑ 26.00 26.01 26.02 26.03 26.04 26.05 26.06 26.07 26.08 26.09 26.10 26.11 26.12 26.13 26.14 26.15 26.16 26.17 26.18 26.19 26.20 26.21 26.22 Gold Report 2021, pp. 8–14, Chapter 1: Definition and overview.
- ↑ 27.0 27.1 27.2 Carlin, BW (July 2023). "Exacerbations of COPD.". Respiratory Care 68 (7): 961–972. doi:10.4187/respcare.10782. PMID 37353338.
- ↑ 28.0 28.1 28.2 28.3 28.4 28.5 28.6 28.7 Voulgareli, I; Antonogiannaki, EM; Bartziokas, K; Zaneli, S; Bakakos, P; Loukides, S; Papaioannou, AI (10 January 2025). "Early Identification of Exacerbations in Patients with Chronic Obstructive Pulmonary Disease (COPD).". Journal of Clinical Medicine 14 (2): 397. doi:10.3390/jcm14020397. PMID 39860403.
- ↑ 29.00 29.01 29.02 29.03 29.04 29.05 29.06 29.07 29.08 29.09 Gold Report 2021, pp. 104–109, Chapter 5: Management of exacerbations.
- ↑ "Common Colds" (in en-us). 7 October 2020. https://www.cdc.gov/features/rhinoviruses/.
- ↑ "Non-typeable Haemophilus influenzae chronic colonization in chronic obstructive pulmonary disease (COPD)". Critical Reviews in Microbiology 47 (2): 192–205. March 2021. doi:10.1080/1040841X.2020.1863330. PMID 33455514.
- ↑ 32.0 32.1 Liu, C; Liu, C; Liu, H; Lin, S (2025). "Characteristics of pathogenic microorganisms in COPD-related infections: prognostic correlations and implications.". Frontiers in Cellular and Infection Microbiology 15. doi:10.3389/fcimb.2025.1739849. PMID 41635718.
- ↑ "Mechanisms of Virus-Induced Airway Immunity Dysfunction in the Pathogenesis of COPD Disease, Progression, and Exacerbation". Frontiers in Immunology 11. 2020. doi:10.3389/fimmu.2020.01205. PMID 32655557.
- ↑ US EPA, OAR (19 April 2016). "Particulate Matter (PM) Basics" (in en). https://www.epa.gov/pm-pollution/particulate-matter-pm-basics#effects.
- ↑ Sacks, JD; Migliaccio, CT; Reid, CE; Montrose, L (14 February 2025). "Shifting the Conversation on Wildland Fire Smoke Exposures: More Smoke Within and Across Years Requires a New Approach to Inform Public Health Action.". ACS ES&T Air 2 (2): 122–129. doi:10.1021/acsestair.4c00236. PMID 40182508. Bibcode: 2025AESTA...2..122S.
- ↑ US EPA, OAR (13 August 2019). "Health Effects Attributed to Wildfire Smoke" (in en). https://www.epa.gov/wildfire-smoke-course/health-effects-attributed-wildfire-smoke.
- ↑ "Forest Fires and Lung Health" (in en). 25 August 2014. https://www.lung.ca/lung-health/air-quality/outdoor-air-quality/forest-fires-and-lung-health.
- ↑ "Bushfire smoke" (in en-AU). 19 March 2014. https://farmerhealth.org.au/2014/03/19/bushfire-smoke.
- ↑ Yang, R; Liu, G; Deng, C (September 2021). "Pulmonary embolism with chronic obstructive pulmonary disease.". Chronic Diseases and Translational Medicine 7 (3): 149–156. doi:10.1016/j.cdtm.2021.04.001. PMID 34505015.
- ↑ "Impact of Frailty on the Risk of Exacerbations and All-Cause Mortality in Elderly Patients with Stable Chronic Obstructive Pulmonary Disease". Clin Interv Aging 16: 593–601. 2021. doi:10.2147/CIA.S303852. PMID 33880018.
- ↑ 41.0 41.1 41.2 41.3 41.4 41.5 41.6 41.7 41.8 Zeng, S; Zhang, Y; Li, S; Li, Z; Li, P; Xie, J; Zhang, J; Xie, L et al. (2025). "From metabolic alterations to chronic inflammation: mechanisms and immunoregulation of metabolic reprogramming in COPD.". Frontiers in Immunology 16. doi:10.3389/fimmu.2025.1698832. PMID 41409289.
- ↑ Wang, Z; Sun, Y (26 February 2024). "Unraveling the causality between chronic obstructive pulmonary disease and its common comorbidities using bidirectional Mendelian randomization.". European Journal of Medical Research 29 (1): 143. doi:10.1186/s40001-024-01686-x. PMID 38403592.
- ↑ 43.0 43.1 43.2 43.3 43.4 43.5 Gold Report 2021, pp. 26–33, Chapter 2: Diagnosis and initial assessment.
- ↑ Gold Report 2021, pp. 121–126, Chapter 6: COPD and comorbidities.
- ↑ 45.0 45.1 45.2 45.3 "Metabolic Syndrome and Air Pollution: A Narrative Review of Their Cardiopulmonary Effects". Toxics 7 (1): 6. January 2019. doi:10.3390/toxics7010006. PMID 30704059. Bibcode: 2019Toxic...7....6C.
- ↑ 46.0 46.1 46.2 "Pulmonary hypertension associated with lung disease: new insights into pathomechanisms, diagnosis, and management". The Lancet. Respiratory Medicine 11 (9): 820–835. September 2023. doi:10.1016/S2213-2600(23)00259-X. PMID 37591300. https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(23)00259-X/abstract.
- ↑ 47.0 47.1 "Pulmonary heart disease: The heart-lung interaction and its impact on patient phenotypes". Pulm Circ 3 (1): 5–19. January 2013. doi:10.4103/2045-8932.109910. PMID 23662171.
- ↑ Dalfardi, B; Abtahi, H; Edalatifard, M; Mozaffari, S; Rahimi, B; Roostaei, G; Khoshnam Rad, N (February 2026). "The Impact of COVID-19 on Obstructive Pulmonary Diseases: A Narrative Review of Long-Term Consequences and Vaccination Strategies.". Health Science Reports 9 (2). doi:10.1002/hsr2.71882. PMID 41737426.
- ↑ "Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease". Am J Respir Crit Care Med 203 (1): 24–36. January 2021. doi:10.1164/rccm.202009-3533SO. PMID 33146552.
- ↑ "Pathobiological mechanisms underlying metabolic syndrome (MetS) in chronic obstructive pulmonary disease (COPD): clinical significance and therapeutic strategies". Pharmacol Ther 198: 160–188. June 2019. doi:10.1016/j.pharmthera.2019.02.013. PMID 30822464.
- ↑ Li, CL; Liu, SF (4 July 2024). "Exploring Molecular Mechanisms and Biomarkers in COPD: An Overview of Current Advancements and Perspectives.". International Journal of Molecular Sciences 25 (13): 7347. doi:10.3390/ijms25137347. PMID 39000454.
- ↑ 52.0 52.1 52.2 52.3 "Genetics of COPD". Annu Rev Physiol 82: 413–431. February 2020. doi:10.1146/annurev-physiol-021317-121224. PMID 31730394.
- ↑ "ICD-11 - ICD-11 for Mortality and Morbidity Statistics". https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1948124976.
- ↑ 54.0 54.1 "6. Chronic Obstructive Pulmonary Disease". Principles of pulmonary medicine (7th ed.). Elsevier. 2019. p. 104. doi:10.1016/B978-0-323-52371-4.00009-X. ISBN 978-0-323-52371-4. https://www.sciencedirect.com/science/article/abs/pii/B978032352371400009X.
- ↑ Manian, P (September 2019). "Chronic obstructive pulmonary disease classification, phenotypes and risk assessment.". Journal of Thoracic Disease 11 (Suppl 14): S1761–S1766. doi:10.21037/jtd.2019.05.10. PMID 31632753.
- ↑ 56.0 56.1 "Imbalance Between Injury and Defense in the COPD Emphysematous Phenotype". Frontiers in Medicine 8. 2021. doi:10.3389/fmed.2021.653332. PMID 34026786.
- ↑ "SMALLa AIRWAY DISEASE IN COPD ASSOCIATED TO BIOMASS EXPOSURE". Rev Invest Clin 71 (1): 70–78. 2019. doi:10.24875/RIC.18002652. PMID 30810542.
- ↑ "Chronic obstructive pulmonary disease and phenotypes: a state-of-the-art". Pulmonology 26 (2): 95–100. 2020. doi:10.1016/j.pulmoe.2019.10.006. PMID 31740261.
- ↑ Mekov, Evgeni; Nuñez, Alexa; Sin, Don D; Ichinose, Masakazu; Rhee, Chin Kook; Maselli, Diego Jose; Coté, Andréanne; Suppli Ulrik, Charlotte et al. (June 2021). "Update on Asthma–COPD Overlap (ACO): A Narrative Review". International Journal of Chronic Obstructive Pulmonary Disease 16: 1783–1799. doi:10.2147/COPD.S312560. PMID 34168440.
- ↑ "Impact of human immunodeficiency virus on pulmonary vascular disease". Glob Cardiol Sci Pract 2021 (2): e202112. June 2021. doi:10.21542/gcsp.2021.12. PMID 34285903.
- ↑ "Airway Epithelium Dysfunction in Cystic Fibrosis and COPD". Mediators Inflamm 2018. 2018. doi:10.1155/2018/1309746. PMID 29849481.
- ↑ "Clinical issues of mucus accumulation in COPD". Int J Chron Obstruct Pulmon Dis 9: 301–2. 2014. doi:10.2147/COPD.S61797. PMID 24741301.
- ↑ 63.0 63.1 "Impact and prevention of severe exacerbations of COPD: a review of the evidence". Int J Chron Obstruct Pulmon Dis 12: 2891–2908. 2017. doi:10.2147/COPD.S139470. PMID 29062228.
- ↑ Beech, A; Higham, A; Booth, S; Tejwani, V; Trinkmann, F; Singh, D (October 2024). "Type 2 inflammation in COPD: is it just asthma?". Breathe (Sheffield, England) 20 (3): 230229. doi:10.1183/20734735.0229-2023. PMID 39534492.
- ↑ 65.0 65.1 Hamanaka, RB; Mutlu, GM (2025-09-02). "Particulate matter air pollution: effects on the respiratory system". The Journal of Clinical Investigation 135 (17). doi:10.1172/JCI194312. ISSN 1558-8238. PMID 40892514.
- ↑ 66.0 66.1 66.2 66.3 66.4 "Chronic obstructive pulmonary disease (COPD) - Aetiology | BMJ Best Practice". https://bestpractice.bmj.com/topics/en-gb/7/aetiology.
- ↑ "Lung development may explain why some non-smokers get COPD and some heavy smokers do not | National Institutes of Health (NIH)" (in en). June 9, 2020. https://www.nih.gov/news-events/news-releases/lung-development-may-explain-why-some-non-smokers-get-copd-some-heavy-smokers-do-not.
- ↑ 68.0 68.1 Chen, Y; Peng, C; Zhang, H; Cai, Y; Yuan, R; Song, P; Zhang, C; Yan, Y (10 February 2023). "Exposure to occupational risk factors is associated with the severity and progression of chronic obstructive pulmonary disease.". Medicine 102 (6). doi:10.1097/MD.0000000000032908. PMID 36820577.
- ↑ "FAQs Dust - Health and Safety Executive (HSE)". https://www.hse.gov.uk/construction/faq-dust.htm.
- ↑ 70.0 70.1 "Treatment of lung disease in alpha-1 antitrypsin deficiency: a systematic review". Int J Chron Obstruct Pulmon Dis 12: 1295–1308. 2017. doi:10.2147/COPD.S130440. PMID 28496314.
- ↑ Khadke, S; Khadke, V; Kumar, A; Makwana, B; Dani, SS; Al-Kindi, S; Rajagopalan, S; Kong, Y et al. (September 2025). "Environmental justice index and prevalence of asthma and COPD in US neighborhoods- a population-based study.". Lancet Regional Health. Americas 49. doi:10.1016/j.lana.2025.101195. PMID 40809452.
- ↑ 72.0 72.1 72.2 Nikolić, MZ; Sun, D; Rawlins, EL (15 August 2018). "Human lung development: recent progress and new challenges.". Development 145 (16). doi:10.1242/dev.163485. PMID 30111617.
- ↑ 73.0 73.1 "Alcohol use disorder: A pre-existing condition for COVID-19?". Alcohol 90: 11–17. February 2021. doi:10.1016/j.alcohol.2020.10.003. PMID 33080339.
- ↑ Ma, Jixuan; Santofimio, Valentina Quintero; Potts, James; Amaral, André F.S. (March 2026). "Alcohol consumption and small airways obstruction". CHEST. doi:10.1016/j.chest.2026.02.019.
- ↑ "[Alcohol consumption and lung damage: Dangerous relationships]" (in French). Rev Mal Respir 35 (10): 1039–1049. December 2018. doi:10.1016/j.rmr.2018.02.009. PMID 29941207.
- ↑ "Effects of different routes of endotoxin injury on barrier function in alcoholic lung syndrome". Alcohol 80: 81–89. November 2019. doi:10.1016/j.alcohol.2018.08.007. PMID 31278041.
- ↑ "The involvement of GM-CSF deficiencies in parallel pathways of pulmonary alveolar proteinosis and the alcoholic lung". Alcohol 80: 73–79. November 2019. doi:10.1016/j.alcohol.2018.07.006. PMID 31229291.
- ↑ 78.0 78.1 78.2 78.3 78.4 78.5 78.6 78.7 Georgakopoulou, VE; Andreikos, DA; Zhu, W; Spandidos, DA (November 2025). "Cannabis use and its impact on respiratory physiology and lung cancer risk: Mechanistic and epidemiological insights (Review).". Biomedical Reports 23 (5): 180. doi:10.3892/br.2025.2058. PMID 41089432.
- ↑ Shabil, M; Malvi, A; Khatib, MN; Ganesan, S; Kaur, M; Srivastava, M; Prasad, GVS; Rajput, P et al. (7 July 2025). "Association of electronic cigarette use and risk of COPD: a systematic review and meta-analysis.". npj Primary Care Respiratory Medicine 35 (1): 31. doi:10.1038/s41533-025-00438-6. PMID 40624045.
- ↑ Hage, R; Fretz, V; Schuurmans, MM (September 2020). "Electronic cigarettes and vaping associated pulmonary illness (VAPI): A narrative review.". Pulmonology 26 (5): 291–303. doi:10.1016/j.pulmoe.2020.02.009. PMID 32553826.
- ↑ 81.0 81.1 Oxford Handbook of Epidemiology for Clinicians. Oxford University Press. 2012. pp. 289–290. ISBN 978-0-19-165478-7. https://books.google.com/books?id=dHLjLwru-l8C&pg=RA1-PT194.
- ↑ Clinical management of chronic obstructive pulmonary disease (2nd ed.). Informa Healthcare. 2013. p. 23. ISBN 978-0-8493-7588-0. https://books.google.com/books?id=DiTThQJkc0UC&pg=PA23.
- ↑ COPD in primary care. Radcliffe Pub.. 2010. p. 9. ISBN 978-1-84619-316-3. https://books.google.com/books?id=CrXFqhezbeMC&pg=PA9.
- ↑ "Host, Gender, and Early-Life Factors as Risks for Chronic Obstructive Pulmonary Disease". Clinics in Chest Medicine 41 (3): 329–337. September 2020. doi:10.1016/j.ccm.2020.06.009. PMID 32800188.
- ↑ "Female Smokers Are at Greater Risk of Airflow Obstruction Than Male Smokers. UK Biobank". American Journal of Respiratory and Critical Care Medicine 195 (9): 1226–1235. May 2017. doi:10.1164/rccm.201608-1545OC. PMID 28075609. https://openaccess.sgul.ac.uk/id/eprint/108529/7/AJRCCM-201608-1545OC-R1_supplement.pdf.
- ↑ "Early life insults as determinants of chronic obstructive pulmonary disease in adult life". International Journal of Chronic Obstructive Pulmonary Disease 13: 683–693. 2018. doi:10.2147/COPD.S153555. PMID 29520136.
- ↑ Eriksson Ström, Jonas; Kebede Merid, Simon; Linder, Robert; Pourazar, Jamshid; Lindberg, Anne; Melén, Erik; Behndig, Annelie F. (2025-01-10). "Airway MMP-12 and DNA methylation in COPD: an integrative approach" (in en). Respiratory Research 26 (1). doi:10.1186/s12931-024-03088-3. ISSN 1465-993X. PMID 39794761.
- ↑ "A Review of the Pulmonary and Health Impacts of Hookah Use". Annals of the American Thoracic Society 16 (10): 1215–1219. October 2019. doi:10.1513/AnnalsATS.201902-129CME. PMID 31091965.
- ↑ 89.0 89.1 89.2 89.3 "Lung Disease Associated With Marijuana Use". Arch Bronconeumol 53 (9): 510–515. September 2017. doi:10.1016/j.arbres.2017.03.019. PMID 28483343.
- ↑ Cherian, SV; Karanth, S; Oldham, SA; Estrada-Y-Martin, RM (January 2026). "Impact of cannabis smoking in patients with COPD: A retrospective cross-sectional study in a safety- net hospital.". Heart & Lung 75: 263–269. doi:10.1016/j.hrtlng.2025.10.011. PMID 41138489.
- ↑ Pradère, P; Marinello, A; Vasseur, D; Naltet, C; Moaca, S; Le Pavec, J; Ghigna, MR; De Montpreville, V et al. (24 September 2025). "The Impact of Dual Cannabis and Tobacco Smoking in Young Patients With Lung Cancer: Results From the Prospective "Environment and Lung Cancer" Study.". Chest 169 (3): 819–829. doi:10.1016/j.chest.2025.09.017. PMID 41005696.
- ↑ "A Systematic Review of the Respiratory Effects of Inhalational Marijuana". Respir Care 61 (11): 1543–1551. November 2016. doi:10.4187/respcare.04846. PMID 27507173.
- ↑ "Access to clean fuels and technologies for cooking". https://ourworldindata.org/grapher/access-to-clean-fuels-and-technologies-for-cooking.
- ↑ 94.0 94.1 94.2 94.3 94.4 94.5 94.6 94.7 Sin, DD; Doiron, D; Agusti, A; Anzueto, A; Barnes, PJ; Celli, BR; Criner, GJ; Halpin, D et al. (May 2023). "Air pollution and COPD: GOLD 2023 committee report.". The European Respiratory Journal 61 (5). doi:10.1183/13993003.02469-2022. PMID 36958741.
- ↑ 95.00 95.01 95.02 95.03 95.04 95.05 95.06 95.07 95.08 95.09 Duan, RR; Hao, K; Yang, T (December 2020). "Air pollution and chronic obstructive pulmonary disease.". Chronic Diseases and Translational Medicine 6 (4): 260–269. doi:10.1016/j.cdtm.2020.05.004. PMID 33336171.
- ↑ Taylor-Blair, HC; Siu, ACW; Haysom-McDowell, A; Kokkinis, S; Bani Saeid, A; Chellappan, DK; Oliver, BGG; Paudel, KR et al. (1 December 2024). "The impact of airborne particulate matter-based pollution on the cellular and molecular mechanisms in chronic obstructive pulmonary disease (COPD).". The Science of the Total Environment 954. doi:10.1016/j.scitotenv.2024.176413. PMID 39322084. Bibcode: 2024ScTEn.95476413T.
- ↑ Bottini, I; Vecchi, S; De Sario, M; Bauleo, L; Trentalange, A; Michelozzi, P; Ancona, C (29 May 2025). "Residential exposure to municipal solid waste incinerators and health effects: a systematic review with meta-analysis.". BMC Public Health 25 (1): 1989. doi:10.1186/s12889-025-23150-z. PMID 40442661.
- ↑ 98.0 98.1 98.2 98.3 Tran, VV; Park, D; Lee, YC (23 April 2020). "Indoor Air Pollution, Related Human Diseases, and Recent Trends in the Control and Improvement of Indoor Air Quality.". International Journal of Environmental Research and Public Health 17 (8): 2927. doi:10.3390/ijerph17082927. PMID 32340311.
- ↑ 99.0 99.1 99.2 99.3 Poole, JA; Zamora-Sifuentes, JL; De Las Vecillas, L; Quirce, S (August 2024). "Respiratory Diseases Associated With Organic Dust Exposure.". The Journal of Allergy and Clinical Immunology. In Practice 12 (8): 1960–1971. doi:10.1016/j.jaip.2024.02.022. PMID 38423290.
- ↑ De Matteis, S; Jarvis, D; Darnton, L; Consonni, D; Kromhout, H; Hutchings, S; Sadhra, SS; Fishwick, D et al. (October 2022). "Lifetime occupational exposures and chronic obstructive pulmonary disease risk in the UK Biobank cohort.". Thorax 77 (10): 997–1005. doi:10.1136/thoraxjnl-2020-216523. PMID 35082144.
- ↑ "COPD Urban-Rural Differences" (in en-us). U.S. Centers for Disease Control and Prevention. May 16, 2024. https://www.cdc.gov/rural-health/php/public-health-strategy/public-health-considerations-for-chronic-obstructive-pulmonary-disease-copd.html.
- ↑ 102.0 102.1 Gaffney, AW; Hawks, L; White, AC; Woolhandler, S; Himmelstein, D; Christiani, DC; McCormick, D (January 2022). "Health Care Disparities Across the Urban-Rural Divide: A National Study of Individuals with COPD.". The Journal of Rural Health 38 (1): 207–216. doi:10.1111/jrh.12525. PMID 33040358.
- ↑ Carlson, SA; Wheaton, AG; Watson, KB; Liu, Y; Croft, JB; Greenlund, KJ (6 May 2022). "Geographic Differences in Sex-Specific Chronic Obstructive Pulmonary Disease Mortality Rate Trends Among Adults Aged ≥25 Years - United States, 1999-2019.". MMWR. Morbidity and Mortality Weekly Report 71 (18): 613–618. doi:10.15585/mmwr.mm7118a1. PMID 35511711.
- ↑ 104.0 104.1 104.2 104.3 "Smoking cessation and environmental hygiene". The Medical Clinics of North America 96 (4): 849–67. July 2012. doi:10.1016/j.mcna.2012.04.014. PMID 22793948.
- ↑ 105.0 105.1 105.2 105.3 105.4 Ortiz-Quintero, B; Martínez-Espinosa, I; Pérez-Padilla, R (23 December 2022). "Mechanisms of Lung Damage and Development of COPD Due to Household Biomass-Smoke Exposure: Inflammation, Oxidative Stress, MicroRNAs, and Gene Polymorphisms.". Cells 12 (1): 67. doi:10.3390/cells12010067. PMID 36611860.
- ↑ Guta, D; Baumgartner, J; Jack, D; Carter, E; Shen, G; Orgill-Meyer, J; Rosenthal, J; Dickinson, K et al. (1 April 2022). "A systematic review of household energy transition in low and middle income countries". Energy Research & Social Science 86. doi:10.1016/j.erss.2021.102463. ISSN 2214-6296. Bibcode: 2022ERSS...8602463G. https://www.sciencedirect.com/science/article/abs/pii/S2214629621005508.
- ↑ Aithal, SS; Sachdeva, I; Kurmi, OP (June 2023). "Air quality and respiratory health in children.". Breathe (Sheffield, England) 19 (2): 230040. doi:10.1183/20734735.0040-2023. PMID 37377853.
- ↑ 108.0 108.1 Blanc, PD; Annesi-Maesano, I; Balmes, JR; Cummings, KJ; Fishwick, D; Miedinger, D; Murgia, N; Naidoo, RN et al. (1 June 2019). "The Occupational Burden of Nonmalignant Respiratory Diseases. An Official American Thoracic Society and European Respiratory Society Statement.". American Journal of Respiratory and Critical Care Medicine 199 (11): 1312–1334. doi:10.1164/rccm.201904-0717ST. PMID 31149852.
- ↑ Pando-Sandoval, A; Ruano-Ravina, A; Candal-Pedreira, C; Rodríguez-García, C; Represas-Represas, C; Golpe, R; Fernández-Villar, A; Pérez-Ríos, M (April 2022). "Risk factors for chronic obstructive pulmonary disease in never-smokers: A systematic review.". The Clinical Respiratory Journal 16 (4): 261–275. doi:10.1111/crj.13479. PMID 35142054.
- ↑ "COPD causes - occupations and substances". https://www.hse.gov.uk/copd/causes.htm#substances.
- ↑ 111.0 111.1 "Genes and chronic obstructive pulmonary disease". The Medical Clinics of North America 96 (4): 699–711. July 2012. doi:10.1016/j.mcna.2012.02.006. PMID 22793939.
- ↑ "Alpha-1 antitrypsin deficiency: a commonly overlooked cause of lung disease". CMAJ 184 (12): 1365–71. September 2012. doi:10.1503/cmaj.111749. PMID 22761482.
- ↑ 113.0 113.1 "Chronic Obstructive Pulmonary Disease". Harrison's Principles of Internal Medicine (18th ed.). McGraw Hill. 2011. pp. 2151–9. ISBN 978-0-07-174889-6.
- ↑ "Home - Gene - NCBI". https://www.ncbi.nlm.nih.gov/gene.
- ↑ "Clinical Epidemiology of COPD: Insights From 10 Years of the COPDGene Study". Chest 156 (2): 228–238. August 2019. doi:10.1016/j.chest.2019.04.135. PMID 31154041.
- ↑ Smith, BM et al. (9 June 2020). "Association of Dysanapsis With Chronic Obstructive Pulmonary Disease Among Older Adults.". JAMA 323 (22): 2268–2280. doi:10.1001/jama.2020.6918. PMID 32515814.
- ↑ "Human airway branch variation and chronic obstructive pulmonary disease". Proc Natl Acad Sci U S A 115 (5): E974–E981. January 2018. doi:10.1073/pnas.1715564115. PMID 29339516. Bibcode: 2018PNAS..115E.974S.
- ↑ Bradding, P; Porsbjerg, C; Côté, A; Dahlén, SE; Hallstrand, TS; Brightling, CE (May 2024). "Airway hyperresponsiveness in asthma: The role of the epithelium.". The Journal of Allergy and Clinical Immunology 153 (5): 1181–1193. doi:10.1016/j.jaci.2024.02.011. PMID 38395082.
- ↑ 119.0 119.1 Suter, P; Greig, R; Chan, R; Lipworth, BJ (January 2026). "Revisiting Type 2 Inflammation and Airway Hyper-responsiveness in COPD.". The Journal of Allergy and Clinical Immunology. In Practice 14 (1): 67–75. doi:10.1016/j.jaip.2025.10.033. PMID 41513335.
- ↑ Kume, H; Yamada, R; Sato, Y; Togawa, R (6 January 2023). "Airway Smooth Muscle Regulated by Oxidative Stress in COPD.". Antioxidants 12 (1): 142. doi:10.3390/antiox12010142. PMID 36671004.
- ↑ 121.0 121.1 Qin, C; Gao, J; Sang, X; Liu, M; Liu, J (December 2025). "Childhood respiratory risk profiles associate with lung function and COPD among the old population.". Annals of Medicine 57 (1). doi:10.1080/07853890.2025.2470954. PMID 40009521.
- ↑ Polverino, F; Sin, DD (February 2026). "The Developmental Origins of Asthma and COPD.". Annual Review of Physiology 88 (1): 513–535. doi:10.1146/annurev-physiol-042924-084007. PMID 40967241.
- ↑ 123.0 123.1 Knight, A (February 2020). "Managing the overlap of asthma and chronic obstructive pulmonary disease.". Australian Prescriber 43 (1): 7–11. doi:10.18773/austprescr.2020.002. PMID 32139956.
- ↑ 124.0 124.1 124.2 Syamlal, G; Dodd, KE; Mazurek, JM (April 2023). "Asthma, chronic obstructive pulmonary disease, and asthma-COPD overlap among US working adults.". The Journal of Asthma 60 (4): 718–726. doi:10.1080/02770903.2022.2089997. PMID 35696621.
- ↑ 125.0 125.1 Brakema, EA; van Gemert, FA; van der Kleij, RMJJ; Salvi, S; Puhan, M; Chavannes, NH (5 March 2019). "COPD's early origins in low-and-middle income countries: what are the implications of a false start?". npj Primary Care Respiratory Medicine 29 (1): 6. doi:10.1038/s41533-019-0117-y. PMID 30837469.
- ↑ Dey, D; Bhattacharyya, P; Roy, D; Saha, D; Sen, S; Ghosh, S; Karmakar, S; Sengupta, S et al. (1 August 2025). "Does childhood TB or pneumonia impact COPD or asthma in adulthood?". The International Journal of Tuberculosis and Lung Disease 29 (8): 349–354. doi:10.5588/ijtld.24.0570. PMID 40751209.
- ↑ Toumpanakis, D; Kim, Y; Usmani, OS (16 July 2025). "Small Airways Disease in Patients With COPD: A Question-and-Answer Approach for Everyday Clinical Practice.". Chest 169 (3): 641–651. doi:10.1016/j.chest.2025.07.002. PMID 40675548.
- ↑ Robbins basic pathology (10th ed.). Elsevier. 2018. pp. 498–502. ISBN 978-0-323-35317-5.
- ↑ "COPD beyond proximal bronchial obstruction: phenotyping and related tools at the bedside". Eur Respir Rev 28 (152): 190010. June 2019. doi:10.1183/16000617.0010-2019. PMID 31285287. PMC 9488991. https://hal.archives-ouvertes.fr/hal-02180604/file/190010.full.pdf.
- ↑ "Assessing Static Lung Hyperinflation by Whole-Body Plethysmography, Helium Dilution, and Impulse Oscillometry System (IOS) in Patients with COPD". Int J Chron Obstruct Pulmon Dis 15: 2583–9. 2020. doi:10.2147/COPD.S264261. PMID 33116475.
- ↑ 131.0 131.1 "Sex differences in severe pulmonary emphysema". American Journal of Respiratory and Critical Care Medicine 176 (3): 243–252. April 2007. doi:10.1164/rccm.200606-828OC. PMID 17431226.
- ↑ "Small airways obstruction and its risk factors in the Burden of Obstructive Lung Disease (BOLD) study: a multinational cross-sectional study". Lancet Glob Health 11 (1): e69–e82. January 2023. doi:10.1016/S2214-109X(22)00456-9. PMID 36521955.
- ↑ "The association of spirometric small airways obstruction with respiratory symptoms, cardiometabolic diseases, and quality of life: results from the Burden of Obstructive Lung Disease (BOLD) study". Respiratory Research 24 (1). 23 May 2023. doi:10.1186/s12931-023-02450-1. PMID 37221593.
- ↑ Knox-Brown, Ben; Potts, James; Santofimio, Valentina Quintero; Minelli, Cosetta; Patel, Jaymini; Abass, Najlaa Mohammed; Agarwal, Dhiraj; Ahmed, Rana et al. (November 2023). "Isolated small airways obstruction predicts future chronic airflow obstruction: a multinational longitudinal study". BMJ Open Respiratory Research 10 (1). doi:10.1136/bmjresp-2023-002056. PMID 37989490.
- ↑ 135.0 135.1 "The pathology of small airways disease in COPD: historical aspects and future directions". Respir Res 20 (1). March 2019. doi:10.1186/s12931-019-1017-y. PMID 30832670.
- ↑ "Airway inflammation in COPD: progress to precision medicine". Eur Respir J 54 (2). August 2019. doi:10.1183/13993003.00651-2019. PMID 31073084. https://figshare.com/articles/journal_contribution/10221875/files/18436544.pdf.
- ↑ "Role of the mucins in pathogenesis of COPD: implications for therapy". Expert Review of Respiratory Medicine 14 (5): 465–483. May 2020. doi:10.1080/17476348.2020.1739525. PMID 32133884.
- ↑ O'Donnell, DE; Milne, KM; James, MD; de Torres, JP; Neder, JA (January 2020). "Dyspnea in COPD: New Mechanistic Insights and Management Implications.". Advances in Therapy 37 (1): 41–60. doi:10.1007/s12325-019-01128-9. PMID 31673990.
- ↑ 139.0 139.1 139.2 "Chronic obstructive pulmonary disease - NICE Pathways". 9 April 2020. https://pathways.nice.org.uk/pathways/chronic-obstructive-pulmonary-disease#path=view%3A/pathways/chronic-obstructive-pulmonary-disease/diagnosing-and-assessing-copd.xml&content=view-node%3Anodes-prognosis-and-severity-assessment.
- ↑ Baldomero, AK; Kunisaki, KM; Bangerter, A; Nelson, DB; Wendt, CH; Fortis, S; Hagedorn, H; Dudley, RA (26 October 2022). "Beyond Access: Factors Associated With Spirometry Underutilization Among Patients With a Diagnosis of COPD in Urban Tertiary Care Centers.". Chronic Obstructive Pulmonary Diseases (Miami, Fla.) 9 (4): 538–548. doi:10.15326/jcopdf.2022.0303. PMID 36040836.
- ↑ 141.0 141.1 Ferrera, MC; Labaki, WW; Han, MK (27 January 2021). "Advances in Chronic Obstructive Pulmonary Disease.". Annual Review of Medicine 72: 119–134. doi:10.1146/annurev-med-080919-112707. PMID 33502902.
- ↑ 142.0 142.1 Blueprints medicine (5th ed.). Wolters Kluwer Health/Lippincott Williams & Wilkins. 2010. p. 69. ISBN 978-0-7817-8870-0. https://books.google.com/books?id=_DHtahEUgXcC&pg=PA69.
- ↑ 143.0 143.1 Maldonado-Franco, A; Giraldo-Cadavid, LF; Tuta-Quintero, E; Bastidas Goyes, AR; Botero-Rosas, DA (2023). "The Challenges of Spirometric Diagnosis of COPD.". Canadian Respiratory Journal 2023. doi:10.1155/2023/6991493. PMID 37808623.
- ↑ 144.0 144.1 144.2 Rodman, Anne (Mar 19, 2024). "COPD: the GOLD 2024 report" (in en). https://practicenurse.co.uk/guidelines/copd-the-gold-2024-report.
- ↑ 145.0 145.1 145.2 Stone, PW; Osen, M; Ellis, A; Coaker, R; Quint, JK (2023). "Prevalence of Chronic Obstructive Pulmonary Disease in England from 2000 to 2019.". International Journal of Chronic Obstructive Pulmonary Disease 18: 1565–1574. doi:10.2147/COPD.S411739. PMID 37497381.
- ↑ 146.0 146.1 Song, JH; Kim, Y (January 2025). "Beyond the Spirometry: New Diagnostic Modalities in Chronic Obstructive Pulmonary Disease.". Tuberculosis and Respiratory Diseases 88 (1): 1–13. doi:10.4046/trd.2024.0040. PMID 39308278.
- ↑ 147.0 147.1 National Institute for Health and Clinical Excellence. Clinical guideline 101: Chronic Obstructive Pulmonary Disease. London, June 2010.
- ↑ "Diagnostic accuracy of screening tools for chronic obstructive pulmonary disease in primary health care: Rapid evidence synthesis". Journal of Family Medicine and Primary Care 10 (6): 2184–2194. June 2021. doi:10.4103/jfmpc.jfmpc_2263_20. PMID 34322411.
- ↑ "The MRC breathlessness scale". Occup Med (Lond) 67 (6): 496–497. August 2017. doi:10.1093/occmed/kqx086. PMID 28898975.
- ↑ "Chronic obstructive pulmonary disease (COPD) - Criteria | BMJ Best Practice". https://bestpractice.bmj.com/topics/en-gb/7/criteria.
- ↑ "COPD Assessment Test (CAT)". American Thoracic Society. http://www.thoracic.org/assemblies/srn/questionaires/copd.php.
- ↑ Lin, Jennifer S.; Webber, Elizabeth M.; Thomas, Rachel G. (May 2022) (in en). Screening for Chronic Obstructive Pulmonary Disease: A Targeted Evidence Update for the U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US). https://www.ncbi.nlm.nih.gov/books/NBK580644/table/ch1.tab1/.
- ↑ Baratella, E; Fiorese, I; Minelli, P; Veiluva, A; Marrocchio, C; Ruaro, B; Cova, MA (2023). "Aging-Related Findings of the Respiratory System in Chest Imaging: Pearls and Pitfalls.". Current Radiology Reports 11 (1): 1–11. doi:10.1007/s40134-022-00405-w. PMID 36471674.
- ↑ Wu, F; Fan, H; Liu, J; Li, H; Zeng, W; Zheng, S; Tian, H; Deng, Z et al. (2021). "Association Between Non-obstructive Chronic Bronchitis and Incident Chronic Obstructive Pulmonary Disease and All-Cause Mortality: A Systematic Review and Meta-Analysis.". Frontiers in Medicine 8. doi:10.3389/fmed.2021.805192. PMID 35145979.
- ↑ 155.0 155.1 155.2 155.3 155.4 Gold Report 2021, pp. 80–83, Chapter 4: Management of stable COPD.
- ↑ 156.0 156.1 156.2 Policy Recommendations for Smoking Cessation and Treatment of Tobacco Dependence. World Health Organization. 2003. pp. 15–40. ISBN 978-92-4-156240-9. https://www.who.int/tobacco/resources/publications/tobacco_dependence/en/.
- ↑ 157.0 157.1 157.2 157.3 Wang, Z; Qiu, Y; Ji, X; Dong, L (2024). "Effects of smoking cessation on individuals with COPD: a systematic review and meta-analysis.". Frontiers in Public Health 12. doi:10.3389/fpubh.2024.1433269. PMID 39722704. Bibcode: 2024FrPH...1233269W.
- ↑ Cunha, AS; Raposo, B; Dias, F; Henriques, S; Martinho, H; Pedro, AR (August 2024). "Management of Chronic Obstructive Pulmonary Disease: Constraints in Patient Pathway and Mitigation Strategies.". Portuguese Journal of Public Health 42 (2): 93–100. doi:10.1159/000535474. PMID 39070594.
- ↑ 159.0 159.1 "Chronic obstructive pulmonary disease in over 16s: diagnosis and management | Guidance and guidelines | NICE". 26 July 2019. https://www.nice.org.uk/guidance/NG115.
- ↑ 160.0 160.1 Li, J; Su, J; Tong, Z; Liang, L (30 May 2025). "Impact of Smoking Cessation Duration on Exacerbation Readmission Frequency and Hospitalization Costs in COPD - Beijing Municipality, China, 2013-2021.". China CDC Weekly 7 (22): 766–770. doi:10.46234/ccdcw2025.126. PMID 40621199.
- ↑ 161.0 161.1 "Smoking cessation and COPD". European Respiratory Review 22 (127): 37–43. March 2013. doi:10.1183/09059180.00007212. PMID 23457163.
- ↑ "Coping with cravings" (in en). 27 April 2018. https://www.nhs.uk/live-well/quit-smoking/stop-smoking-coping-with-cravings/.
- ↑ "Smoking cessation for people with chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2019 (8). August 2016. doi:10.1002/14651858.CD010744.pub2. PMID 27545342.
- ↑ Howard, J; Schulte, PA (February 2026). "Preventing and Managing Chronic Disease in the Work Environment: Using the Total Worker Health Approach.". American Journal of Industrial Medicine 69 (2): 82–88. doi:10.1002/ajim.70042. PMID 41342494.
- ↑ 165.0 165.1 Su, X; Gu, H; Li, F; Shi, D; Wang, Z (2023). "Global, Regional, and National Burden of COPD Attributable to Occupational Particulate Matter, Gases, and Fumes, 1990-2019: Findings from the Global Burden of Disease Study 2019.". International Journal of Chronic Obstructive Pulmonary Disease 18: 2971–2983. doi:10.2147/COPD.S436879. PMID 38111466.
- ↑ Bongers, Q; Comellas, AP (1 March 2025). "Impact of occupational exposures in patients with chronic obstructive pulmonary disease: current understanding and knowledge gaps.". Current Opinion in Pulmonary Medicine 31 (2): 98–105. doi:10.1097/MCP.0000000000001141. PMID 39564609.
- ↑ "31. Occupational Exposure as a Cause of Chronic Airways Disease §Prevention of Work-Related COPD". Environmental and occupational medicine (4th ed.). Wolters Kluwer/Lippincott Williams & Wilkins. 2007. pp. 521–2. ISBN 978-0-7817-6299-1. https://books.google.com/books?id=H4Sv9XY296oC&pg=PA521.
- ↑ Anlimah, F; Gopaldasani, V; MacPhail, C; Davies, B (April 2023). "A systematic review of the effectiveness of dust control measures adopted to reduce workplace exposure.". Environmental Science and Pollution Research International 30 (19): 54407–54428. doi:10.1007/s11356-023-26321-w. PMID 36964805. Bibcode: 2023ESPR...3054407A.
- ↑ Nassikas, NJ; McCormack, MC; Ewart, G; Balmes, JR; Bond, TC; Brigham, E; Cromar, K; Goldstein, AH et al. (March 2024). "Indoor Air Sources of Outdoor Air Pollution: Health Consequences, Policy, and Recommendations: An Official American Thoracic Society Workshop Report.". Annals of the American Thoracic Society 21 (3): 365–376. doi:10.1513/AnnalsATS.202312-1067ST. PMID 38426826.
- ↑ Rawat, N; Kumar, P (1 February 2023). "Interventions for improving indoor and outdoor air quality in and around schools.". The Science of the Total Environment 858 (Pt 2). doi:10.1016/j.scitotenv.2022.159813. PMID 36411671. Bibcode: 2023ScTEn.85859813R.
- ↑ McCarron, A; Semple, S; Braban, CF; Swanson, V; Gillespie, C; Price, HD (May 2023). "Public engagement with air quality data: using health behaviour change theory to support exposure-minimising behaviours.". Journal of Exposure Science & Environmental Epidemiology 33 (3): 321–331. doi:10.1038/s41370-022-00449-2. PMID 35764891. Bibcode: 2023JESEE..33..321M.
- ↑ "City Launches First-in-the-Nation 'Breathe Philly' Network to Bring Real-Time Air Quality Data to Every Neighborhood | Department of Public Health" (in en). City of Philadelphia. 22 February 2026. https://www.phila.gov/2026-02-18-city-launches-first-in-the-nation-breathe-philly-network-to-bring-real-time-air-quality-data-to-every-neighborhood/.
- ↑ Evangelopoulos, D; Chatzidiakou, L; Walton, H; Katsouyanni, K; Kelly, FJ; Quint, JK; Jones, RL; Barratt, B (July 2021). "Personal exposure to air pollution and respiratory health of COPD patients in London.". The European Respiratory Journal 58 (1). doi:10.1183/13993003.03432-2020. PMID 33542053.
- ↑ Yang, Y; Goh, KY; Teo, HH; Tan, SS (10 September 2024). "The Impact of Air Pollution Information on Individuals' Exercise Behavior: Empirical Study Using Wearable and Mobile Devices Data.". JMIR mHealth and uHealth 12. doi:10.2196/55207. PMID 39255029.
- ↑ 175.0 175.1 Ipek, Ö; Ipek, E (December 2021). "Effects of indoor air pollution on household health: evidence from Turkey.". Environmental Science and Pollution Research International 28 (47): 67519–67527. doi:10.1007/s11356-021-15175-9. PMID 34258706. Bibcode: 2021ESPR...2867519I.
- ↑ "Chronic obstructive pulmonary disease (COPD) - Treatment - NHS". 20 October 2017. https://www.nhs.uk/conditions/chronic-obstructive-pulmonary-disease-copd/treatment/.
- ↑ 177.0 177.1 Sun, Y; Zhou, J (2019). "New insights into early intervention of chronic obstructive pulmonary disease with mild airflow limitation.". International Journal of Chronic Obstructive Pulmonary Disease 14: 1119–1125. doi:10.2147/COPD.S205382. PMID 31213792.
- ↑ CDC (2024-01-18). "RSV information for healthcare providers" (in en-us). https://www.cdc.gov/rsv/clinical/index.html.
- ↑ Cravo, A; Attar, D; Freeman, D; Holmes, S; Ip, L; Singh, SJ (2022). "The Importance of Self-Management in the Context of Personalized Care in COPD.". International Journal of Chronic Obstructive Pulmonary Disease 17: 231–243. doi:10.2147/COPD.S343108. PMID 35095272.
- ↑ Lenferink, A; Brusse-Keizer, MGJ; van der Palen, J; Effing, TW (2025). "Personalizing Self-Management Interventions in COPD - Looking Beyond One-Size-Fits-All.". International Journal of Chronic Obstructive Pulmonary Disease 20: 65–68. doi:10.2147/COPD.S511278. PMID 39802034.
- ↑ "Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2017 (8). August 2017. doi:10.1002/14651858.CD011682.pub2. PMID 28777450.
- ↑ 182.0 182.1 182.2 182.3 182.4 182.5 Gold Report 2021, pp. 60–65, Chapter 3: Evidence supporting prevention and maintenance therapy.
- ↑ "Vitamin D to prevent exacerbations of COPD: systematic review and meta-analysis of individual participant data from randomised controlled trials". Thorax 74 (4): 337–345. April 2019. doi:10.1136/thoraxjnl-2018-212092. PMID 30630893.
- ↑ 184.0 184.1 "Antibiotics for exacerbations of chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2018 (10). October 2018. doi:10.1002/14651858.CD010257.pub2. PMID 30371937.
- ↑ 185.0 185.1 Putcha, N; Wise, RA (June 2018). "Medication Regimens for Managing COPD Exacerbations.". Respiratory Care 63 (6): 773–782. doi:10.4187/respcare.05912. PMID 29794210.
- ↑ 186.0 186.1 186.2 186.3 Janjua, S; Mathioudakis, AG; Fortescue, R; Walker, RA; Sharif, S; Threapleton, CJ; Dias, S (15 January 2021). "Prophylactic antibiotics for adults with chronic obstructive pulmonary disease: a network meta-analysis.". The Cochrane Database of Systematic Reviews 1 (1). doi:10.1002/14651858.CD013198.pub2. PMID 33448349.
- ↑ "Fluoroquinolone Antibacterial Drugs: Drug Safety Communication – FDA Advises Restricting Use for Certain Uncomplicated Infections". 12 May 2016. https://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm500665.htm.
- ↑ "Association of Home Noninvasive Positive Pressure Ventilation With Clinical Outcomes in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis". JAMA 323 (5): 455–465. February 2020. doi:10.1001/jama.2019.22343. PMID 32016309.
- ↑ Chawla, R; Dixit, SB; Zirpe, KG; Chaudhry, D; Khilnani, GC; Mehta, Y; Khatib, KI; Jagiasi, BG et al. (January 2020). "ISCCM Guidelines for the Use of Non-invasive Ventilation in Acute Respiratory Failure in Adult ICUs.". Indian Journal of Critical Care Medicine 24 (Suppl 1): S61–S81. doi:10.5005/jp-journals-10071-G23186. PMID 32205957.
- ↑ 190.0 190.1 "Chronic obstructive pulmonary disease". Lancet 379 (9823): 1341–51. April 2012. doi:10.1016/S0140-6736(11)60968-9. PMID 22314182. Bibcode: 2012Lanc..379.1341D.
- ↑ "Palliative care in pulmonary medicine" (in Portuguese). Jornal Brasileiro de Pneumologia 46 (3). 2020. doi:10.36416/1806-3756/e20190280. PMID 32638839.
- ↑ Bronchodilators. StatPearls Publishing. 2021. PMID 30085570. https://www.ncbi.nlm.nih.gov/books/NBK519028/. Retrieved 27 July 2021.
- ↑ 193.0 193.1 193.2 Gold Report 2021, pp. 48–52, Chapter 3: Evidence supporting prevention and maintenance therapy.
- ↑ 194.0 194.1 "Chronic obstructive pulmonary disease in over 16s: diagnosis and management". 5 December 2018. https://www.nice.org.uk/guidance/ng115/chapter/Recommendations.
- ↑ 195.0 195.1 195.2 Miravitlles, M; Kawayama, T; Dreher, M (8 November 2022). "LABA/LAMA as First-Line Therapy for COPD: A Summary of the Evidence and Guideline Recommendations.". Journal of Clinical Medicine 11 (22): 6623. doi:10.3390/jcm11226623. PMID 36431099.
- ↑ "Dual combination therapy versus long-acting bronchodilators alone for chronic obstructive pulmonary disease (COPD): a systematic review and network meta-analysis". The Cochrane Database of Systematic Reviews 2018 (12). December 2018. doi:10.1002/14651858.CD012620.pub2. PMID 30521694.
- ↑ Li, X; Zheng, J; Luo, D; Liu, R (30 January 2024). "The optimal dose of indacaterol for treatment of chronic obstructive pulmonary disease: a systematic review and Bayesian network meta-analysis.". Journal of Thoracic Disease 16 (1): 344–355. doi:10.21037/jtd-23-1044. PMID 38410541.
- ↑ Buhl, R; Miravitlles, M; Anzueto, A; Brunton, S (January 2024). "Long-acting muscarinic antagonist and long-acting β(2)-agonist combination for the treatment of maintenance therapy-naïve patients with chronic obstructive pulmonary disease: a narrative review.". Therapeutic Advances in Respiratory Disease 18. doi:10.1177/17534666241279115. PMID 39352722.
- ↑ 199.0 199.1 Fukuda, Nobuhiko; Horita, Nobuyuki; Kaneko, Ayami; Goto, Atsushi; Kaneko, Takeshi; Ota, Erika; Kew, Kayleigh M. (2023-06-05). "Long-acting muscarinic antagonist (LAMA) plus long-acting beta-agonist (LABA) versus LABA plus inhaled corticosteroid (ICS) for stable chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2023 (6). doi:10.1002/14651858.CD012066.pub3. ISSN 1469-493X. PMID 37276335.
- ↑ 200.0 200.1 Huang, YJ; Wang, KY; Chien, WC; Chung, CH; Kao, LT; Kao, S; Chian, CF (2025). "Paradigm Shift in the Treatment of Chronic Obstructive Pulmonary Disease Improves Patient Outcomes.". International Journal of Chronic Obstructive Pulmonary Disease 20: 1965–1972. doi:10.2147/COPD.S511593. PMID 40551760.
- ↑ "Triple therapy in the management of chronic obstructive pulmonary disease: systematic review and meta-analysis". BMJ 363. November 2018. doi:10.1136/bmj.k4388. PMID 30401700.
- ↑ 202.0 202.1 Anzueto, A; Miravitlles, M (29 July 2020). "Tiotropium in chronic obstructive pulmonary disease - a review of clinical development.". Respiratory Research 21 (1): 199. doi:10.1186/s12931-020-01407-y. PMID 32727455.
- ↑ de Miguel-Diez, J; Albaladejo-Vicente, R; Palacios-Ceña, D; Carabantes-Alarcon, D; Zamorano-Leon, JJ; Lopez-Herranz, M; Lopez-de-Andres, A (9 December 2020). "The Impact of COPD in Trends of Urinary Tract Infection Hospitalizations in Spain, 2001-2018: A Population-Based Study Using Administrative Data.". Journal of Clinical Medicine 9 (12): 3979. doi:10.3390/jcm9123979. PMID 33316870.
- ↑ Aisanov, Z; Khaltaev, N (May 2020). "Management of cardiovascular comorbidities in chronic obstructive pulmonary disease patients.". Journal of Thoracic Disease 12 (5): 2791–2802. doi:10.21037/jtd.2020.03.60. PMID 32642187.
- ↑ Gomes, F; Cheng, SL (5 March 2023). "Pathophysiology, Therapeutic Targets, and Future Therapeutic Alternatives in COPD: Focus on the Importance of the Cholinergic System.". Biomolecules 13 (3): 476. doi:10.3390/biom13030476. PMID 36979411.
- ↑ "Umeclidinium bromide versus placebo for people with chronic obstructive pulmonary disease (COPD)". The Cochrane Database of Systematic Reviews 2017 (6). June 2017. doi:10.1002/14651858.CD011897.pub2. PMID 28631387.
- ↑ "Comparative efficacy of long-acting muscarinic antagonist monotherapies in COPD: a systematic review and network meta-analysis". International Journal of Chronic Obstructive Pulmonary Disease 10: 2495–517. 2015. doi:10.2147/COPD.S92412. PMID 26604738.
- ↑ 208.0 208.1 "Inhaled Corticosteroids and the Pneumonia Risk in Patients With Chronic Obstructive Pulmonary Disease: A Meta-analysis of Randomized Controlled Trials". Front Pharmacol 12. 2021. doi:10.3389/fphar.2021.691621. PMID 34267661.
- ↑ "[The place of inhaled corticosteroids in COPD]". Revue des Maladies Respiratoires 33 (10): 877–891. December 2016. doi:10.1016/j.rmr.2015.11.009. PMID 26831345.
- ↑ "Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2014 (9). September 2014. doi:10.1002/14651858.CD001288.pub4. PMID 25178099.
- ↑ "Different durations of corticosteroid therapy for exacerbations of chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2018 (3). March 2018. doi:10.1002/14651858.CD006897.pub4. PMID 29553157.
- ↑ van Geffen, Wouter H.; Tan, Daniel J.; Walters, Julia A.E.; Walters, E. Haydn (2023-12-06). Cochrane Airways Group. ed. "Inhaled corticosteroids with combination inhaled long-acting beta2-agonists and long-acting muscarinic antagonists for chronic obstructive pulmonary disease". Cochrane Database of Systematic Reviews 2023 (12). doi:10.1002/14651858.CD011600.pub3. PMID 38054551.
- ↑ 213.0 213.1 213.2 213.3 213.4 213.5 Gold Report 2021, pp. 54–58, Chapter 3: Evidence supporting prevention and maintenance therapy.
- ↑ 214.0 214.1 214.2 214.3 214.4 214.5 214.6 Tran, AT; Ghanem, AS; Móré, M; Nagy, AC; Tóth, Á (21 November 2024). "Efficacy of Prophylactic Antibiotics in COPD: A Systematic Review.". Antibiotics 13 (12): 1110. doi:10.3390/antibiotics13121110. PMID 39766500.
- ↑ 215.0 215.1 "Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD)". The Cochrane Database of Systematic Reviews 2018 (10). October 2018. doi:10.1002/14651858.CD009764.pub3. PMID 30376188.
- ↑ "Mucolytic agents versus placebo for chronic bronchitis or chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 5 (3). May 2019. doi:10.1002/14651858.CD001287.pub6. PMID 31107966.
- ↑ "Erdosteine". https://bnf.nice.org.uk/drug/erdosteine.html.
- ↑ "Mucus, Microbiomes and Pulmonary Disease". Biomedicines 9 (6): 675. June 2021. doi:10.3390/biomedicines9060675. PMID 34199312.
- ↑ "Bronchitis" (in en). 17 October 2017. https://www.nhs.uk/conditions/bronchitis/.
- ↑ "Role of metformin in treatment of patients with chronic obstructive pulmonary disease: a systematic review". Journal of Thoracic Disease 11 (10): 4371–4378. October 2019. doi:10.21037/jtd.2019.09.84. PMID 31737323.
- ↑ 221.0 221.1 "Oxygen therapy in COPD and interstitial lung disease: navigating the knowns and unknowns". ERJ Open Res 5 (3). July 2019. doi:10.1183/23120541.00118-2019. PMID 31544111.
- ↑ "Oxygen for breathlessness in patients with chronic obstructive pulmonary disease who do not qualify for home oxygen therapy". The Cochrane Database of Systematic Reviews 11 (8). November 2016. doi:10.1002/14651858.CD006429.pub3. PMID 27886372.
- ↑ Chronic Obstructive Pulmonary Disease. Jaypee Brothers Medical. 2013. p. 139. ISBN 978-93-5090-353-7. https://books.google.com/books?id=PTgIAQAAQBAJ&pg=PA139.
- ↑ 224.0 224.1 "BTS guideline for emergency oxygen use in adult patients". Thorax 63 (6): vi1-68. October 2008. doi:10.1136/thx.2008.102947. PMID 18838559.
- ↑ Venkatesan, Priya (January 2024). "GOLD COPD report: 2024 update" (in en). The Lancet Respiratory Medicine 12 (1): 15–16. doi:10.1016/S2213-2600(23)00461-7. PMID 38061380. https://linkinghub.elsevier.com/retrieve/pii/S2213260023004617.
- ↑ "Pulmonary Rehabilitation". https://medlineplus.gov/pulmonaryrehabilitation.html.
- ↑ "Water-based exercise training for chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews (12). December 2013. doi:10.1002/14651858.CD008290.pub2. PMID 24353107.
- ↑ "Non-invasive ventilation during exercise training for people with chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2014 (5). May 2014. doi:10.1002/14651858.CD007714.pub2. PMID 24823712.
- ↑ 229.0 229.1 "Upper limb exercise training for COPD". The Cochrane Database of Systematic Reviews 2016 (11). November 2016. doi:10.1002/14651858.CD011434.pub2. PMID 27846347.
- ↑ 230.0 230.1 "Tai Chi for chronic obstructive pulmonary disease (COPD)". The Cochrane Database of Systematic Reviews 2016 (6). June 2016. doi:10.1002/14651858.CD009953.pub2. PMID 27272131.
- ↑ Ammous, Omar; Feki, Walid; Lotfi, Tamara; Khamis, Assem M; Gosselink, Rik; Rebai, Ahmed; Kammoun, Samy (2023-01-06). Cochrane Airways Group. ed. "Inspiratory muscle training, with or without concomitant pulmonary rehabilitation, for chronic obstructive pulmonary disease (COPD)" (in en). Cochrane Database of Systematic Reviews 2023 (1). doi:10.1002/14651858.CD013778.pub2. PMID 36606682.
- ↑ "The impact of home-based physiotherapy interventions on breathlessness during activities of daily living in severe COPD: a systematic review". Physiotherapy 96 (2): 108–19. June 2010. doi:10.1016/j.physio.2009.09.006. PMID 20420957.
- ↑ 233.0 233.1 "The Use of Spinal Manipulative Therapy in the Management of Chronic Obstructive Pulmonary Disease: A Systematic Review". Journal of Alternative and Complementary Medicine 22 (2): 108–14. February 2016. doi:10.1089/acm.2015.0199. PMID 26700633.
- ↑ "Effectiveness of manual therapy in COPD: A systematic review of randomised controlled trials". Pulmonology 25 (4): 236–247. 2019. doi:10.1016/j.pulmoe.2018.12.008. PMID 30738792.
- ↑ 235.0 235.1 "Airway clearance techniques for chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2012 (3). March 2012. doi:10.1002/14651858.CD008328.pub2. PMID 22419331.
- ↑ "Nutritional supplementation for stable chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2012 (12). December 2012. doi:10.1002/14651858.CD000998.pub3. PMID 23235577.
- ↑ "Bronchodilators delivered by nebuliser versus inhalers for lung attacks of chronic obstructive pulmonary disease". Cochrane Database of Systematic Reviews 29 (8): 011826. 29 August 2016. doi:10.1002/14651858.CD011826.pub2. PMID 27569680.
- ↑ "Chronic Obstructive Pulmonary Disease (COPD)". Pulmonary Disorders: Merck Manuals Professional Edition. https://www.merckmanuals.com/professional/pulmonary-disorders/chronic-obstructive-pulmonary-disease-and-related-disorders/chronic-obstructive-pulmonary-disease-copd.
- ↑ "Home warmth and health status of COPD patients". Eur. J. Public Health 18 (4): 399–405. 2008. doi:10.1093/eurpub/ckn015. PMID 18367496.
- ↑ "Synergistic effects of temperature and humidity on the symptoms of COPD patients". Int J Biometeorol 61 (11): 1919–25. 2017. doi:10.1007/s00484-017-1379-0. PMID 28567499. Bibcode: 2017IJBm...61.1919M.
- ↑ "Humidifiers: Ease skin, breathing symptoms". Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/common-cold/in-depth/humidifiers/art-20048021.
- ↑ "High humidity leads to loss of infectious influenza virus from simulated coughs". PLOS ONE 8 (2). 2013. doi:10.1371/journal.pone.0057485. PMID 23460865. Bibcode: 2013PLoSO...857485N.
- ↑ 243.0 243.1 Gold Report 2021, pp. 92–96, Chapter 4: Management of stable COPD.
- ↑ "Surgical and endoscopic interventions that reduce lung volume for emphysema: a systemic review and meta-analysis". The Lancet. Respiratory Medicine 7 (4): 313–324. April 2019. doi:10.1016/S2213-2600(18)30431-4. PMID 30744937. https://pure.rug.nl/ws/files/81829213/1_s2.0_S2213260018304314.pdf.
- ↑ 245.0 245.1 "Surgical Therapies for Chronic Obstructive Pulmonary Disease". Clinics in Chest Medicine 41 (3): 559–566. September 2020. doi:10.1016/j.ccm.2020.06.011. PMID 32800206.
- ↑ 246.0 246.1 "1 Recommendations | Endobronchial valve insertion to reduce lung volume in emphysema | Guidance | NICE". 20 December 2017. https://www.nice.org.uk/guidance/ipg600/chapter/1-Recommendations.
- ↑ "Endobronchial Valves for the Treatment of Advanced Emphysema". Chest 159 (5): 1833–1842. May 2021. doi:10.1016/j.chest.2020.12.007. PMID 33345947.
- ↑ "Lung volume reduction with endobronchial coils for patients with emphysema". J Thorac Dis 10 (Suppl 23): S2797–S2805. August 2018. doi:10.21037/jtd.2017.12.95. PMID 30210833.
- ↑ "Bronchoscopic Thermal Vapour Ablation: Hot Stuff to Treat Emphysema Patients!". Archivos de Bronconeumologia 53 (1): 1–2. January 2017. doi:10.1016/j.arbr.2016.11.009. PMID 27916315.
- ↑ "Lung Scintigraphy in COPD". Seminars in Nuclear Medicine 49 (1): 16–21. January 2019. doi:10.1053/j.semnuclmed.2018.10.010. PMID 30545511.
- ↑ "WHO Disease and injury country estimates". World Health Organization. 2009. https://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html.
- ↑ 252.0 252.1 "Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010". Lancet 380 (9859): 2197–2223. December 2012. doi:10.1016/S0140-6736(12)61689-4. PMID 23245608.
- ↑ "Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010". Lancet 380 (9859): 2163–2196. December 2012. doi:10.1016/S0140-6736(12)61729-2. PMID 23245607.
- ↑ 254.0 254.1 "COPD prevalence". https://cks.nice.org.uk/topics/chronic-obstructive-pulmonary-disease/background-information/prevalence-incidence/.
- ↑ 255.0 255.1 255.2 255.3 255.4 Wang, Z; Cao, W; You, Z; Li, S; Xue, M; Li, H; Lin, J; Cai, G et al. (August 2025). "Factors influencing the prevalence and death rate of COPD: a pan-database ecological study covering 201 countries and regions from 1990 to 2021.". eClinicalMedicine 86. doi:10.1016/j.eclinm.2025.103347. PMID 40791891.
- ↑ Naeem, S; Wang, F; Mubarak, R; Shen, H; Li, X; Mommers, I; Hussain, SR; Malik, SS et al. (7 April 2025). "Mapping the Global distribution, risk factors, and temporal trends of COPD incidence and mortality (1990-2021): ecological analysis.". BMC Medicine 23 (1): 210. doi:10.1186/s12916-025-04014-0. PMID 40197280.
- ↑ 257.0 257.1 ((GBD 2021 Causes of Death Collaborators)) (18 October 2025). "Global burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.". Lancet 406 (10513): 1811–1872. doi:10.1016/S0140-6736(25)01917-8. PMID 41092928.
- ↑ "The top 10 causes of death" (in en). Fact Sheets. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
- ↑ 259.0 259.1 Mei, F; Dalmartello, M; Bonifazi, M; Bertuccio, P; Levi, F; Boffetta, P; Negri, E; La Vecchia, C et al. (November 2022). "Chronic obstructive pulmonary disease (COPD) mortality trends worldwide: An update to 2019.". Respirology 27 (11): 941–950. doi:10.1111/resp.14328. PMID 35831204.
- ↑ "Basics About COPD" (in en-us). Chronic Obstructive Pulmonary Disease (COPD). Center for Disease Control. 9 June 2021. https://www.cdc.gov/copd/basics-about.html.
- ↑ Bazell, C; Alston, M; Feigler, N; Germack, HD; Leary, S; Fopalan, W; Mannino, D (27 March 2025). "Variation in Prevalence and Burden of Chronic Obstructive Pulmonary Disease by State and Insurance Type in the United States.". Chronic Obstructive Pulmonary Diseases 12 (2): 158–174. doi:10.15326/jcopdf.2024.0560. PMID 40147474.
- ↑ 262.0 262.1 262.2 262.3 262.4 262.5 "The history of COPD". International Journal of Chronic Obstructive Pulmonary Disease 1 (1): 3–14. 2006. doi:10.2147/copd.2006.1.1.3. PMID 18046898.
- ↑ 263.0 263.1 "Pathologic Features of Chronic Obstructive Pulmonary Disease: Diagnostic Criteria and Differential Diagnosis". Fishman's Pulmonary Diseases and Disorders (4th ed.). McGraw-Hill. 2008. pp. 693–705. ISBN 978-0-07-164109-8. http://www.mhprofessional.com/downloads/products/0071457399/0071457399_chap40.pdf. Retrieved 2008-11-11.
- ↑ "The Search for Words to Describe the Bad Blowers". Chest 85 (6): 73S–74S. 1984. doi:10.1378/chest.85.6_Supplement.73S.
- ↑ A struggle with Titans. Carlton Press. 1965. p. 6. https://books.google.com/books?id=hLRpAAAAMAAJ.
- ↑ "One hundred years of chronic obstructive pulmonary disease". American Journal of Respiratory and Critical Care Medicine 171 (9): 941–8. May 2005. doi:10.1164/rccm.200412-1685OE. PMID 15849329.
- ↑ "November is National COPD Awareness Month | NHLBI, NIH". https://www.nhlbi.nih.gov/health-topics/education-and-awareness/copd-learn-more-breathe-better/copd-awareness-month.
- ↑ 268.0 268.1 Global problems, local solutions: costs and benefits. Cambridge University Press. 2013. p. 143. ISBN 978-1-107-03959-9. https://books.google.com/books?id=cRZaAQAAQBAJ&pg=PA143.
- ↑ The Global Economic Burden of Noncommunicable Diseases. World Economic Forum. 2011. p. 24. http://www3.weforum.org/docs/WEF_Harvard_HE_GlobalEconomicBurdenNonCommunicableDiseases_2011.pdf.
- ↑ "COPD commissioning toolkit". https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/212876/chronic-obstructive-pulmonary-disease-COPD-commissioning-toolkit.pdf.
- ↑ "Stem cell therapy for chronic obstructive pulmonary disease". Chin Med J (Engl) 134 (13): 1535–1545. June 2021. doi:10.1097/CM9.0000000000001596. PMID 34250959.
- ↑ "Intravenous alpha-1 antitrypsin augmentation therapy for treating patients with alpha-1 antitrypsin deficiency and lung disease". The Cochrane Database of Systematic Reviews 2016 (9). September 2016. doi:10.1002/14651858.CD007851.pub3. PMID 27644166.
- ↑ Gea, Joaquim; Enríquez-Rodríguez, César J.; Agranovich, Bella; Pascual-Guardia, Sergi (2023). "Update on metabolomic findings in COPD patients". ERJ Open Research 9 (5): 00180–2023. doi:10.1183/23120541.00180-2023. ISSN 2312-0541. PMID 37908399.
- ↑ Dasgupta, Sanjukta; Ghosh, Nilanjana; Bhattacharyya, Parthasarathi; Roy Chowdhury, Sushmita; Chaudhury, Koel (2023-02-17). "Metabolomics of asthma, COPD, and asthma-COPD overlap: an overview" (in en). Critical Reviews in Clinical Laboratory Sciences 60 (2): 153–170. doi:10.1080/10408363.2022.2140329. ISSN 1040-8363. PMID 36420874.
- ↑ Zeng, Xiaoyin; Lan, Yanting; Xiao, Jing; Hu, Longbo; Tan, Long; Liang, Mengdi; Wang, Xufei; Lu, Shaohua et al. (2022-12-02). "Advances in phosphoproteomics and its application to COPD" (in en). Expert Review of Proteomics 19 (7–12): 311–324. doi:10.1080/14789450.2023.2176756. ISSN 1478-9450. PMID 36730079.
- ↑ "Telehealthcare for chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews 2012 (7). July 2011. doi:10.1002/14651858.CD007718.pub2. PMID 21735417. PMC 8939044. http://discovery.dundee.ac.uk/ws/files/1821515/Telehealthcare_for_chronic_obstructive_pulmonary_disease.pdf.
- ↑ "Developing a patient-driven chronic obstructive pulmonary disease (COPD) research agenda in the U.S.". Journal of Patient-Reported Outcomes 5 (1). December 2021. doi:10.1186/s41687-021-00399-7. PMID 34865193.
- ↑ Anatomy and Physiology of Domestic Animals. Wiley. 2008. p. 852. ISBN 978-1-118-70115-7. https://books.google.com/books?id=Ze6J2znDg38C&pg=PT852.
- ↑ "Recurrent Airway Obstruction in Horses - Respiratory System" (in en). https://www.msdvetmanual.com/respiratory-system/respiratory-diseases-of-horses/recurrent-airway-obstruction-in-horses.
- ↑ "Cardiopulmonary disease in the geriatric dog and cat". The Veterinary Clinics of North America. Small Animal Practice 19 (1): 87–102. January 1989. doi:10.1016/S0195-5616(89)50007-X. PMID 2646821.
Works cited
- Global Strategy for Prevention, Diagnosis and Management of COPD: 2021 Report. Global Initiative for Chronic Obstructive Lung Disease. 25 November 2020. https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf. Retrieved 28 June 2021.
External links
- WHO fact sheet on COPD
- "COPD". MedlinePlus. U.S. National Library of Medicine. https://medlineplus.gov/copd.html.
| Classification | |
|---|---|
| External resources |
 |  |

{kind=link}